Article Text

Abstract
Introduction/Background The TCGA molecular classification of endometrial cancer (EC) has proven prognostic impact for patients with intermediate-risk EC. The randomised PORTEC-3 trial investigated the benefit of combined adjuvant chemotherapy and radiotherapy (CTRT) compared with RT alone for women with high-risk EC (HREC). We evaluated the prognostic significance of the molecular classification in HREC using tissues from consenting PORTEC-3 trial participants.
Methodology 423 paraffin-embedded tissue samples (64% of 660 participants) were collected. Through targeted DNA-sequencing for pathogenic POLE-exonuclease domain mutations (EDM) and immunohistochemistry for p53 and mismatch repair (MMR) proteins, the HREC were classified as POLE-ultramutated (POLEmut), p53 mutant staining (p53abn), MMR-deficient (MMRd) or no specific molecular profile (NSMP). The Kaplan-Meier method, log-rank test and Cox’s proportional hazard model were used for analysis.
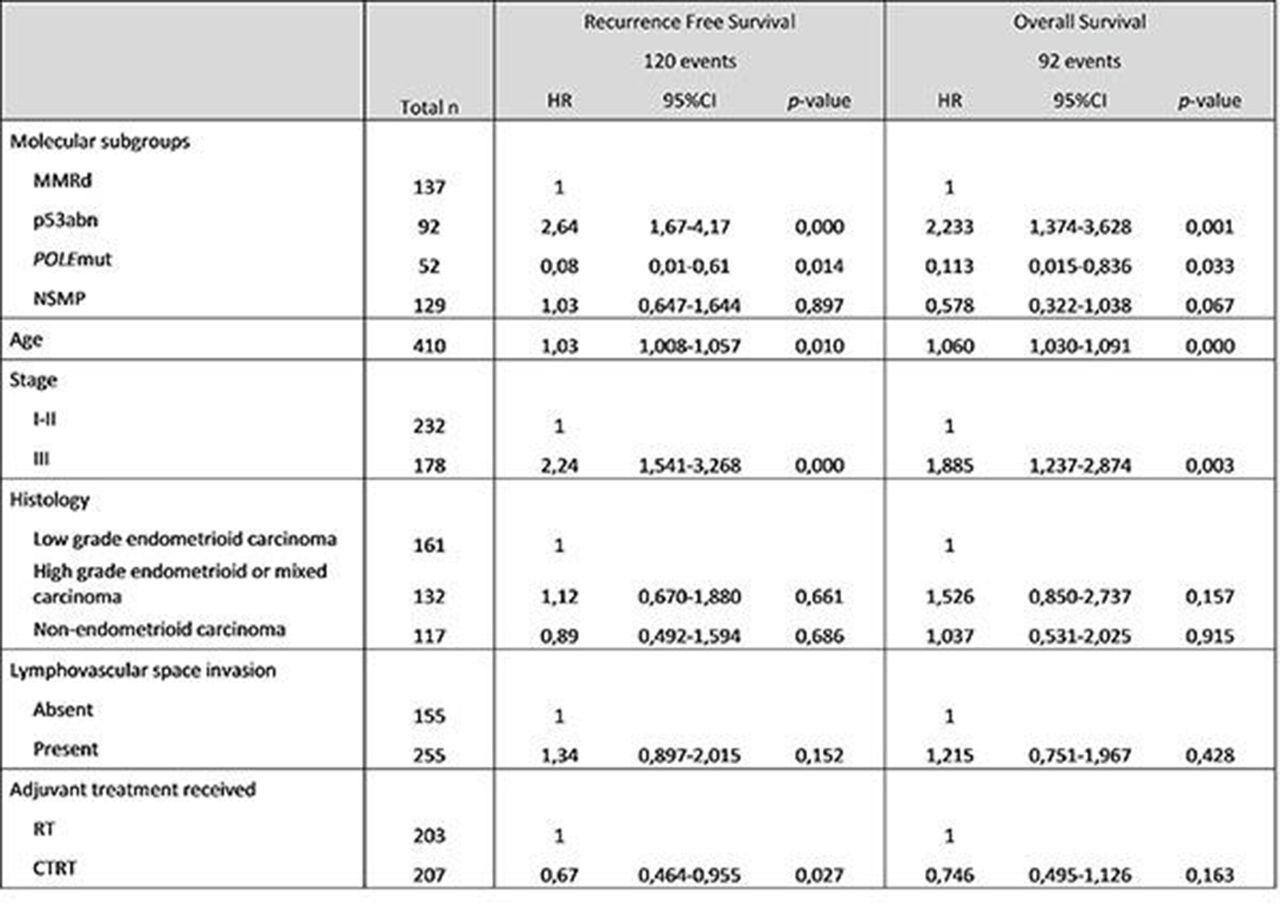
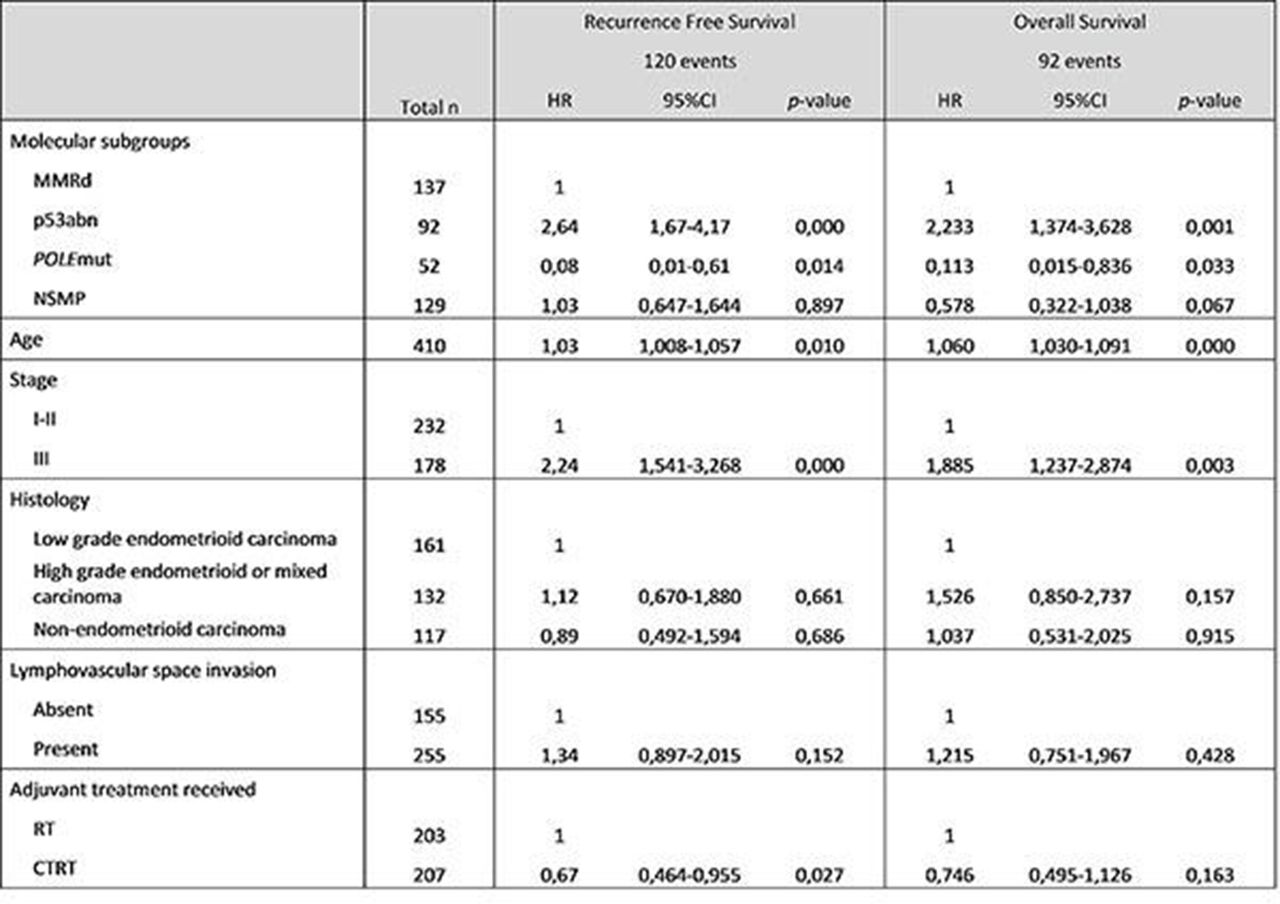
Results Molecular analysis was successful in 410 HREC (97% of the 423), identifying 4 molecular subgroups: p53abn (n=92, 22%), POLEmut (n=52, 13%), MMRd (n=137, 33%) and NSMP (n=129, 32%). Five-year recurrence-free survival (RFS) for patients with POLEmut, p53abn, MMRd and NSMP EC was 98%, 50%, 74% and 76%, respectively (p<0.0001), and overall survival was 98%, 55%, 81% and 88% (p<0.0001). Multivariable analysis showed that p53abn was the strongest prognostic factor for decreased survival, while pathogenic POLE EDM was the strongest favourable factor (table 1). Patients with p53abn HREC had significant benefit of combined adjuvant chemotherapy and radiotherapy (5-year RFS with CTRT 61% versus 37% for RT, log-rank p=0.015).
{kind=link}
Multivariable analysis of molecular subgroups and clinicopathological features (n=410)
Conclusion The molecular classification provides better risk stratification than histopathology alone. Patients with POLEmut HREC have excellent clinical outcome, suggesting these should be classified as low-risk, independent of other pathologic variables. P53abn EC is the strongest predictor of poor clinical outcome, and these patients had significant benefit from added chemotherapy. Molecular characteristics should be incorporated in clinical diagnostics and decision making and future trials should address molecular subgroup-based treatments.
Disclosure AL reports receiving advisory board fees from AstraZeneca, Tesaro, Clovis, MSD, Grisdstone, Seattle Genetics, Gamamabs, and Biocad, and travel support paid to her institution from Roche and AstraZeneca. HN reports is the founder of SME Vicinivax and has collaborated with Aduro, TRON & Merck.