Article Text

Abstract
Introduction/Background During excision of bulky lymph nodes, there is an increased risk of operative vessel injury.
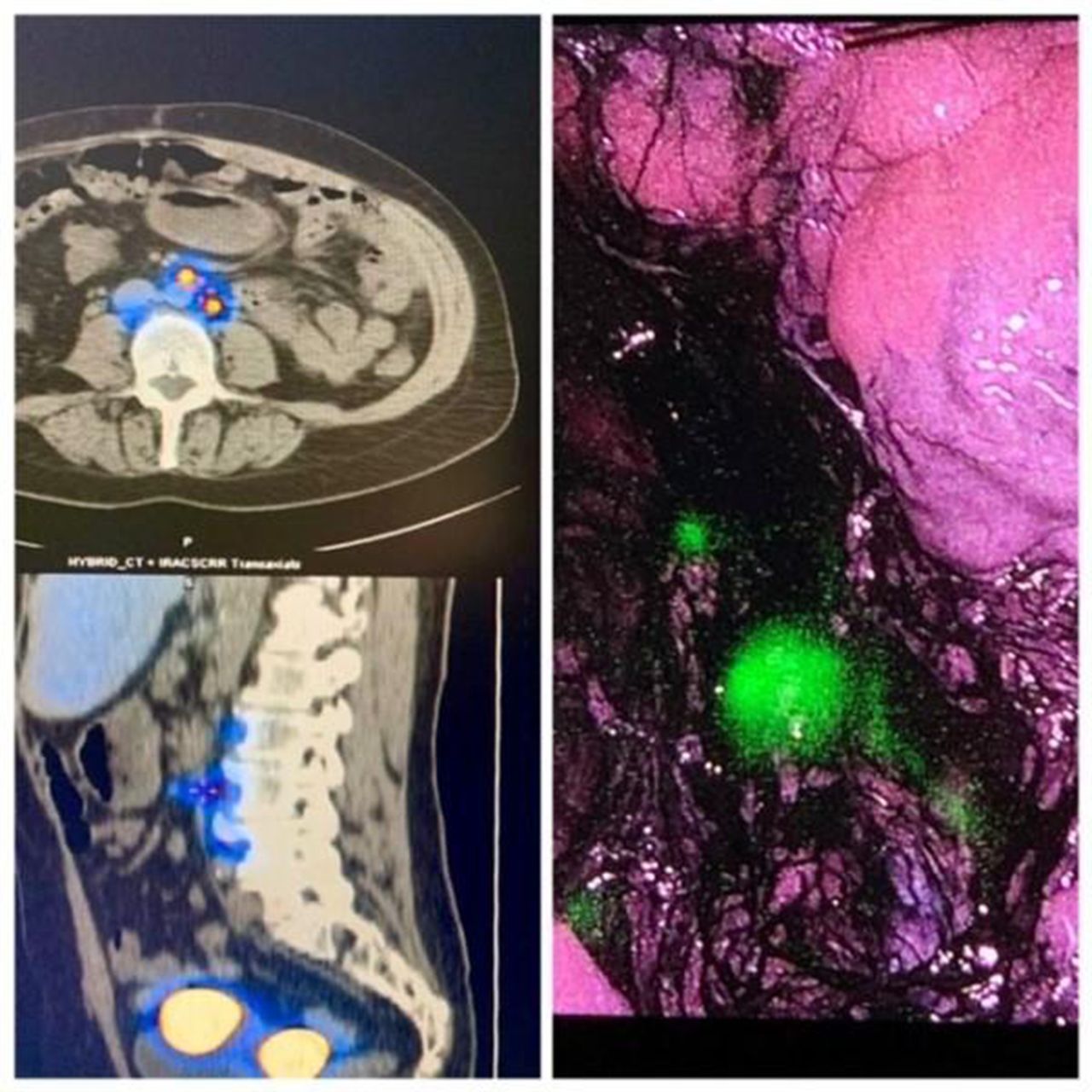
Methodology 59 years old woman with a preoperative endometrial biopsy result of Grade 3 endometrioid endometrial cancer admitted to the Gynecologic Oncology clinic with the abdominal computed tomography result which indicates bulky lymph nodes at the paraaortic retrocaval region.
Results Entering the retroperitoneal paraaortic area by cutting the peritoneum with an incision beginning below the cecum and extending along the base of small bowel mesentery up to the level of ligament of Treitz (suspensory muscle of duodenum).
Small bowels are kept outside the surgical field; right lateral traction of ascending colon and right ureter, cranial traction of duodenum and left lateral traction of mesentery of sigmoid colon.
At the level of L3-L4 vertebra; inferior vena cava is isolated and retracted over the bulky lymph node. Tape traction of inferior vena cava from the superior and inferior part of bulky lymph node facilitates the surgery and provides a hemostatic control.
A cleavage is developed on the right border of inferior vena cava and the bulky lymph node is excised from the retrocaval and inter aortocaval space.

{kind=link}
{kind=link}
Conclusion Meticulous dissection with proper surgical and anatomic landmarks is extremely important in resection of bulky lymph nodes especially if they are located on the retrocaval or retroaortic region.
Disclosure Nothing to disclose