Article Text

Abstract
Methodology A 68-year-old gravida 7, para 5 woman with body mass index of 41 was admitted to our clinic for postmenopausal bleeding. The result of an endometrial biopsy was endometrioid adenocarcinoma with grade 3. Laparoscopic hysterectomy, bilateral salpingoooferectomy, infracolic omentectomy, pelvic and paraaortic lymphadenectomy was performed.
Results In this video, we report an immediate repair of an incompletely lacerated inferior vena cava during laparoscopic paraaortic lymphadenectomy in a patient with endometrial cancer. After injury, lacerated edges of inferior vena cava were held by two graspers and approximated wit 5/0 polypropylene suture.Beside this, we aim to present following errors during management of vascular bleeding i; improper use of irrigator aspirator system during control of minor vascular bleeding by electrothermal bipolar tissue sealing system ii; how improper intraabdominal cleaning of telescope leads to waste of time and massive bleeding iii; how careless suppression of an irrigator aspirator instrument above the level of cauterized edge of inferior vena cava leads to laceration of inferior vena cava.
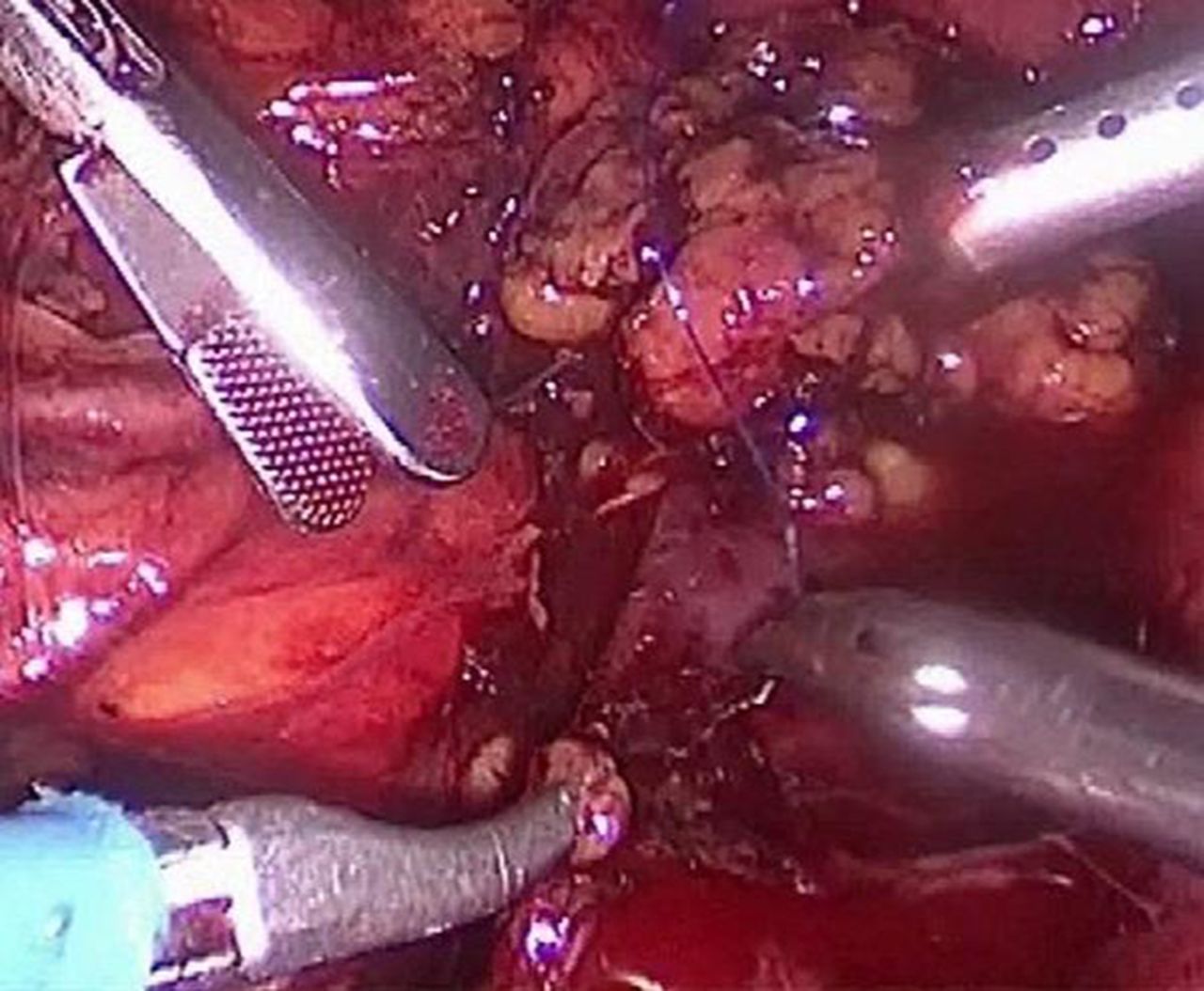
Suturing inferior vena cava injury

{kind=link}
{kind=link}
Final view of paraaortic lymphadenectomy
Conclusion Laparoscopic surgery of endometrial cancer requiring lymphadenectomy should only be managed by experienced and skillful laparoscopic surgeons with extensive knowledge about vascular surgery.
Disclosure Nothing to disclose