Article Text

Abstract
Introduction/Background Extensive surgery has been shown in retrospective studies to improve survival from advanced ovarian cancer. UK uptake of extensive surgery has been variable, owing to concerns regarding the impact on quality of life (QoL) and organizational factors. We investigated QoL after surgery in parallel, multicentre, international, prospective cohorts, here reporting UK and Kolkata, India results.
Methodology Patients completed EORTC-QLQ-C30 and other Patient Reported Outcome Measures pre-operation and at 6 weeks, 6, 12, 18 and 24 month postoperatively. Surgical complexity scores (SCS), intraoperative disease load and survival up to two years were collected and Kaplan Meier survival analyses and forward stepwise Cox proportional hazard models of overall survival conducted. The association of SCS with QLQ-C30 global scores at 6 weeks, 6 months and 12 months post-surgery was evaluated using general linear repeated measures models (SPSS 24).
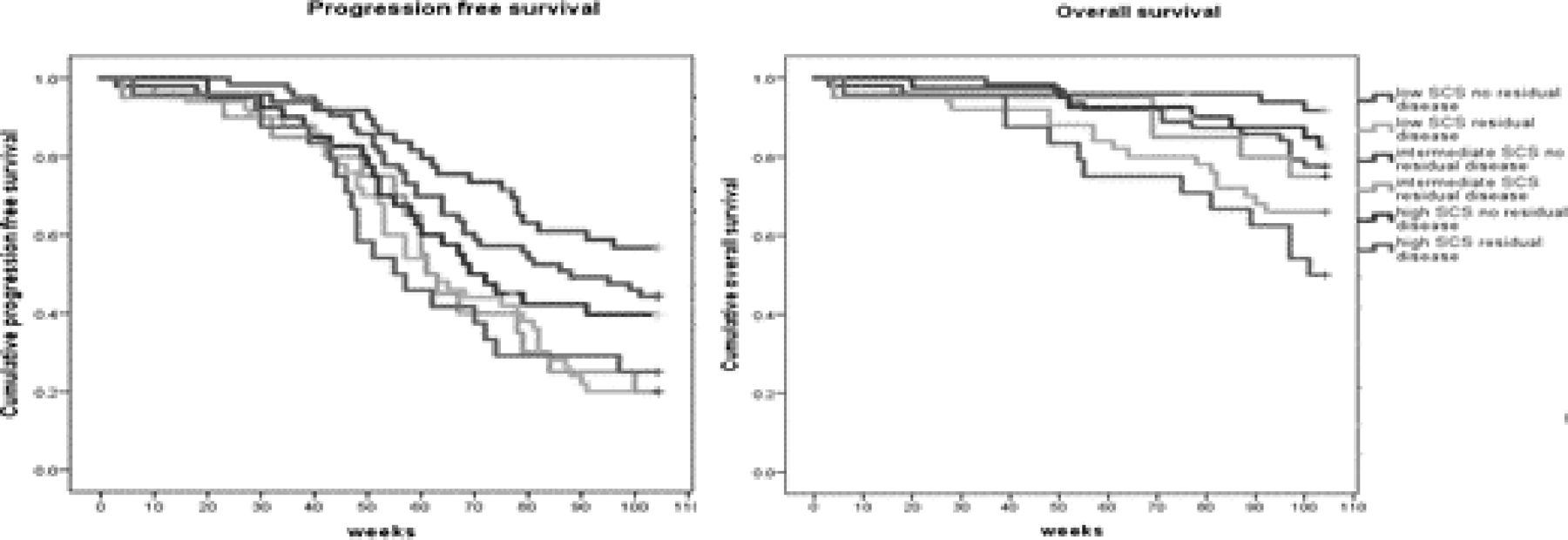
Results In 247 patients, those undergoing high (64) or intermediate (70) SCS procedures were younger, showed better performance status, higher disease load, more upper abdominal disease and greater cytoreduction rates although all SCS groups included patients with a higher burden of disease. (Table 1). Progression free and overall survival was poorer with residual disease in all SCS groups (log rank p≤0.001) (figure 1). Age Adjusted Charlson Comorbidity Index, pre-operative albumin and Peritoneal Carcinomatosis Index were independent predictors of survival (table 2). In a complete case analysis, post operation QLQ-C30 improved in all SCS groups between 6 weeks and 12 months (p<0.001) (figure 2) with no statistically significant or large differences between SCS groups over that time.
Conclusion In this observational study, QoL of patients improved postoperatively, and was no worse in patients undergoing complex surgery during that period. Extensive surgery to achieve complete cytoreduction for high disease load was associated with improved survival and no deleterious impact on QoL in the post operative year.
Disclosure Nothing to disclose
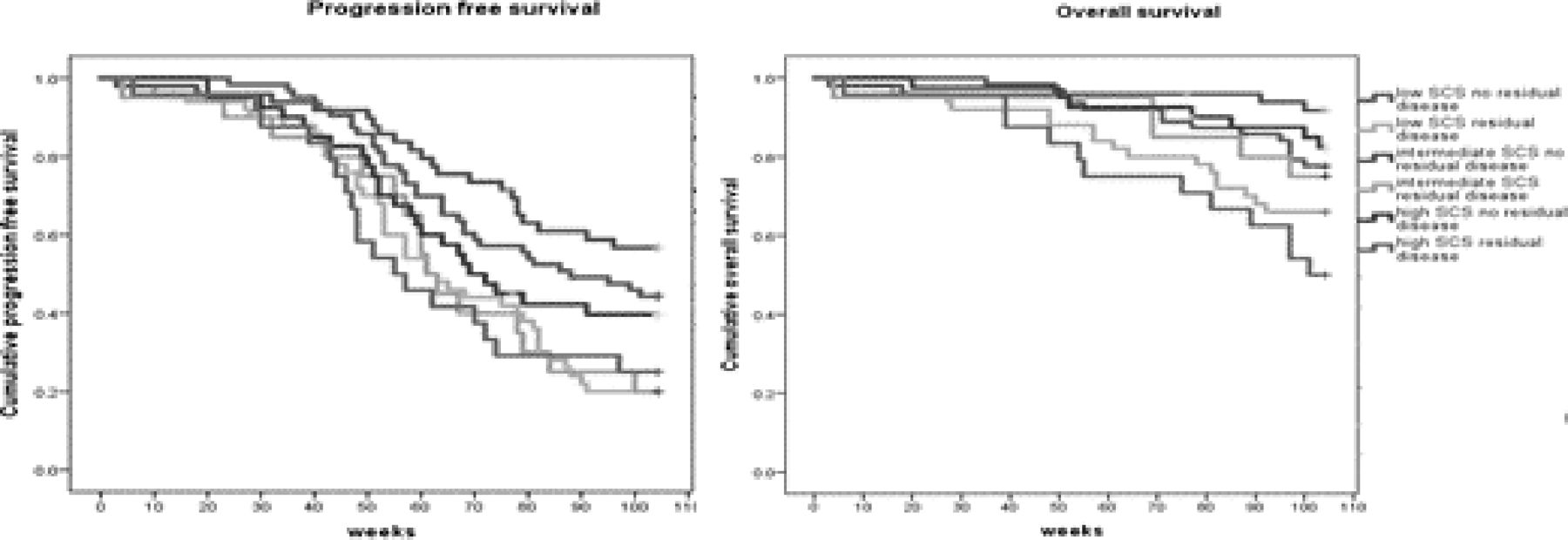
Survival by Surgical Complexity Score and by presence of residual disease

{kind=link}
{kind=link}
EORTC30 Global scores by surgical complexity score in patients without disease progression
Patient characteristics by Surgical Complexity Score (SCS)
Overall survival adjusted hazard ratios (Cox proportional hazards)