Article Text

Abstract
Introduction/Background Pelvic lymph node metastasis carries the highest impact on decreased survival among surgical-pathological risk factors for early-stage cervical cancer. The goal of this study was to examine the association between the use of concurrent chemotherapy and survival in women with early-stage cervical cancer and nodal metastasis receiving adjuvant radiotherapy.
Methodology This is a population-based cohort study using the Surveillance, Epidemiology, and End Results Program from 1988–2016. Women with stage T1-2 cervical cancer with pelvic lymph node metastasis who underwent hysterectomy and received postoperative radiotherapy were examined. Trends, characteristics, and overall survival (OS) were compared between women who received postoperative radiotherapy alone (n=729) or in combination with CCRT (n=1,809). Propensity score-based inverse probability of treatment weighting (PS-IPTW) was used to account for the effect of measured covariates on treatment selection.
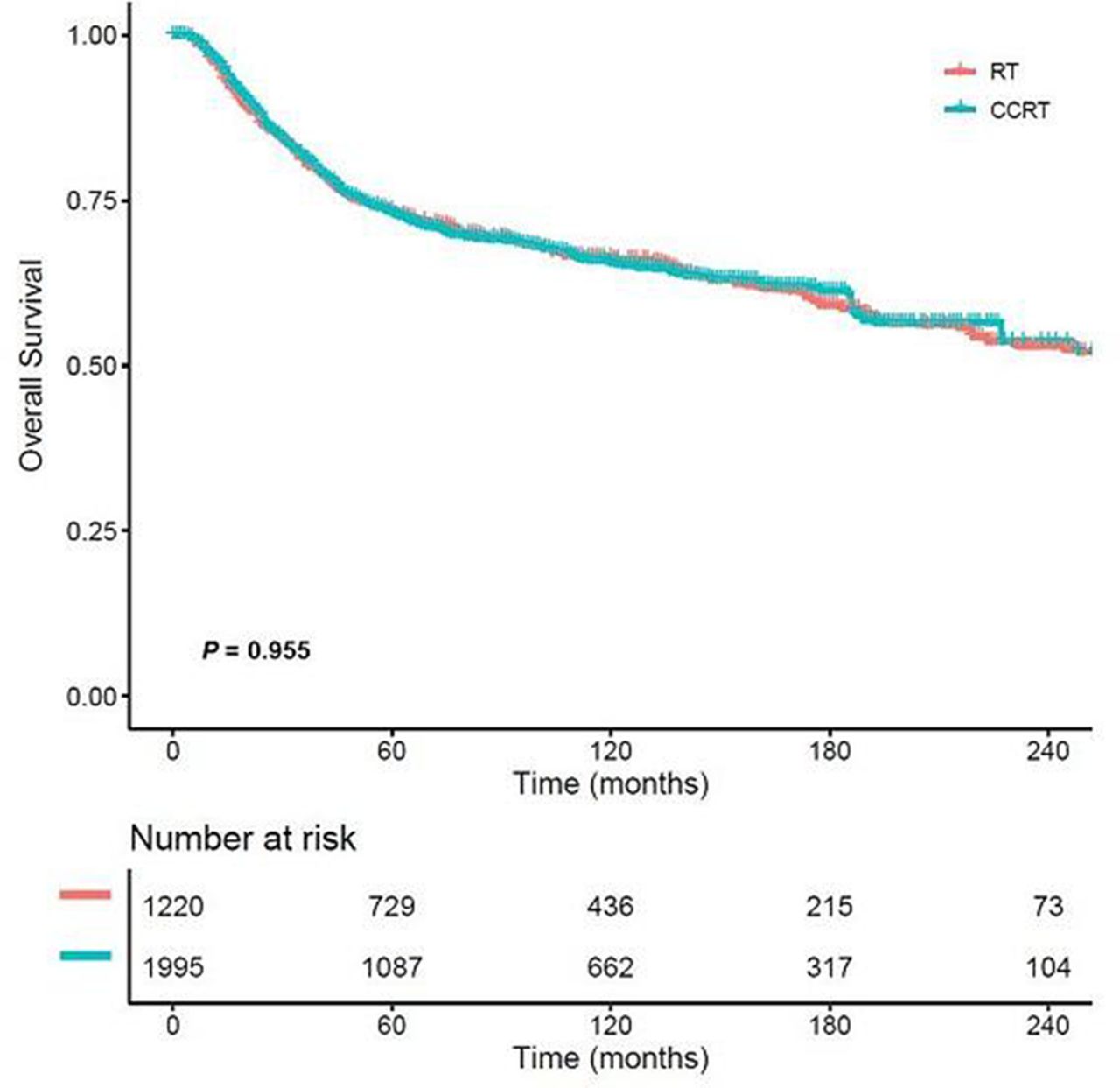
Results Among 2,538 women, there was a marked increase in the use of concurrent chemotherapy from 1997–2000 (20.7% to 78.5%, P=0.052) followed by a more gradual rise through 2016 (88.3%, P<0.001). In a multivariable model, women with non-squamous cell carcinomas and those diagnosed more recently were more likely to receive CCRT, while older women were less likely to receive CCRT (all, P<0.05). At the population level, the 5-year OS rates remained unchanged (annual percent change for 1997–2012 -0.1, 95% confidence interval [CI] -1.2 to 1.0, P=0.776). In a propensity score weighted cohort, women who received CCRT had a 5-year OS rate similar to those treated with radiotherapy alone (73.1% versus 73.6%, hazard ratio 1.004, 95%CI 0.887–1.136, P=0.955). Significant differences were also not seen in older women, non-squamous types, stage T2 disease, and multiple node metastases (all, P>0.05).
Conclusion Despite the marked increase in the use of CCRT for women with early-stage cervical cancer and nodal metastases, there was no association between use of concurrent chemotherapy during postoperative radiotherapy and improved survival.
Disclosure Consultant, Tesaro and Clovis Oncology, research funding Merck (J.D.W.); consultant, Quantgene (L.D.R.); honorarium, Chugai, book editorial expense, Springer, and investigator meeting attendance expense, VBL therapeutics (K.M.); none for others.

{kind=link}
Post-operative OS rates stage T1-2, N1 cervical cancer pts undergoing RT (n=729) or CCRT (n=1,809)