Article Text

Abstract
Introduction/Background Treatment of advanced epithelial ovarian cancer (EOC) requires an accurate estimation of surgical complexity and residual disease (RD) at primary debulking surgery (PDS). Neoadjuvant chemotherapy (NACT) may be used in non-surgical candidates. However, reaching the interval debulking surgery (IDS) will not be possible in all cases. How do we choose the best option in each case? What are our results?
Methodology We included stage IIIC/IV EOC patients undergoing PDS from 2005 to 2016. We collected different variables: Age, Performance Status, Stage, CA 125, type of treatment and residual disease (RD). Overall survival (OS) was estimated using the Kaplan-Meier method.
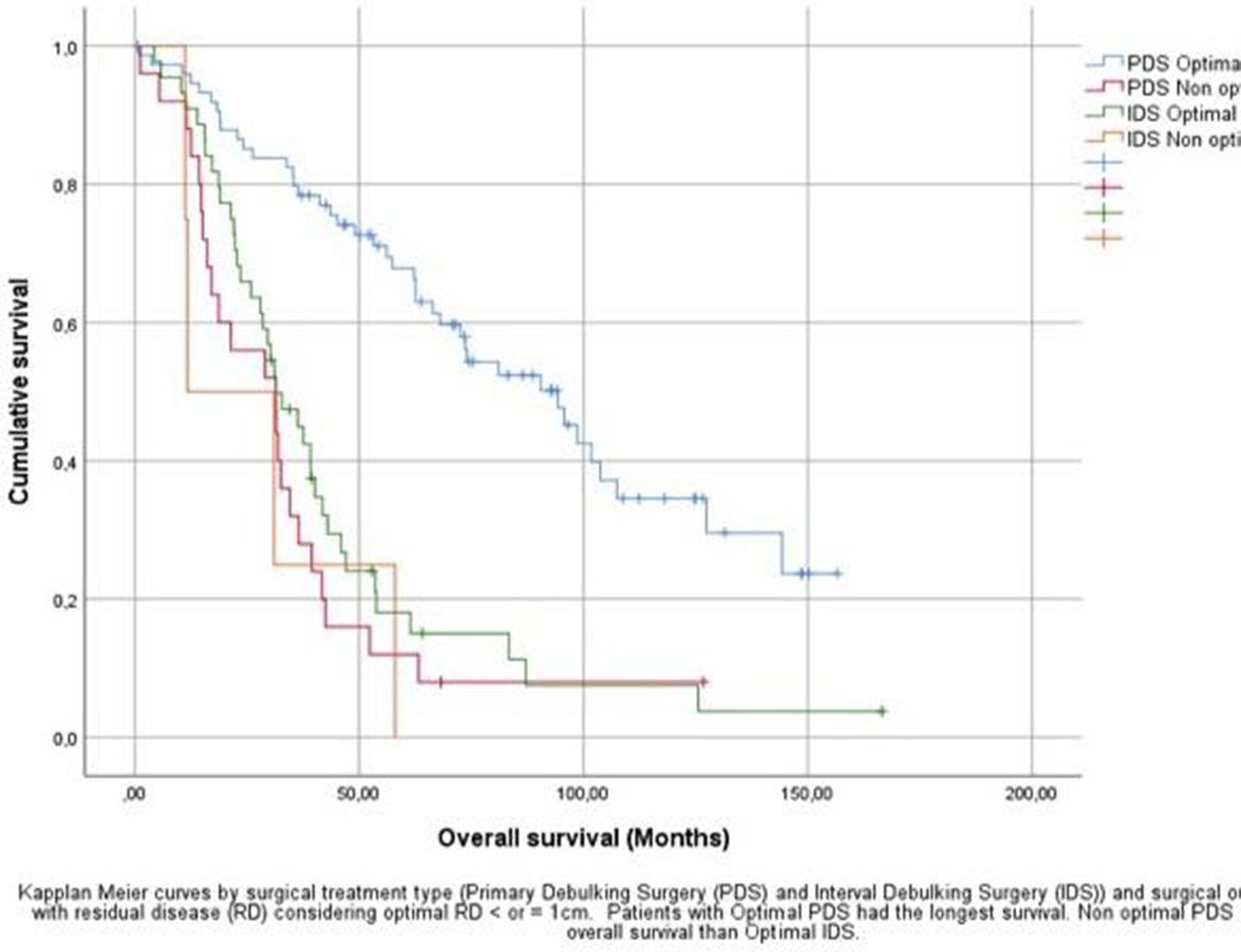
Results A total of 394 patients were diagnosed with EOC, 216 with IIIC/IV stages were recruited in this study. Average age was 64.7 years and the most common histologic type (88.4%) was serous. Up to 15.3% of the cohort was treated with Palliative Care, 36.7% NACT and 48% with PDS (figure 1). Worst performance status and oldest patients were treated with chemotherapy or palliative care (table 1). Optimal PDS was achieved in 80.7% while Optimal IDS was possible in 96.3%. Although the length-of-stay was similar, the complexity of the surgery and the later morbidity was higher in PDS compared to IDS (table 2). Patients with optimal PDS and and Optimal IDS had an OS of 81.1 and 31.4 months respectively, while non optimal PDS obtained an OS of 29 months. (figure 2).

Flow diagram of patients with EOC in Navarre between 2005–2016
Comparison of initial characteristics among treatment groups
Primary debulking surgery vs interval debulking surgery. Outcomes

{kind=link}
{kind=link}
Kaplan Meier curves. PDS vs IDS Survival according to residual disease
Conclusion Advanced EOC treatment was adapted according to patients clinical characteristics. There was a clear survival advantage for PDS group. Nevertheless, non optimal PDS increase morbidity without advantages in survival compared to IDS. Further studies are needed to improve the selection criteria for PDS.
Disclosure Nothing to disclose.