Article Text

Abstract
Introduction/Background Lateral pelvic side wall involvement by gynecological malignancies has been considered for a long time an absolute contraindication to curative resection. Recently the surgical paradigm is challenged with the development of the Laterally Extended Endopelvic Resection, LEER. Although the LEER is perfectly standardized in open surgery, just one small experience has been published about its endoscopic feasibility.The objective of this study is to analyze the feasibility of Laparoscopically Modified Laterally Extended Endopelvic Resection, LM-LEER, in patients with gynecological malignancies involving the lateral pelvic side wall.
Methodology We retrospectively evaluated a consecutive series of women submitted, between July 2014 and November 2018, to LM-LEER for gynecological tumors involving the pelvic side wall. Surgical and post-operative data were analyzed.
Results Overall, 39 women received LEER due to gynecological cancer infiltrating the pelvic side wall, of them 18 (46.2%) were eligible for laparoscopic approach. No laparotomic conversions were registered. In all patients R0 resection was achieved with negative margins of surgical resection at final histological evaluation. The median operative time was 415 min (285–615 min), estimated blood loss was 285 ml (100–600 ml) and the median length of hospital stay was 10 days (4–22 days). There were three (16.7%) intraoperative complications, all managed laparoscopically. In two (11.1%) cases a second surgical exploration was required, one for hemoperitoneum and another for vaginal cuff dehiscence.
Conclusion LM-LEER can be safely performed in carefully selected patients with gynecological malignancies involving the lateral pelvic side wall, in particular for those in which a bladder and rectal sparing surgery appears possible. Further larger prospective trials are needed to evaluate the oncological and the long-term functional outcome of patients undergoing LM-LEER.
Disclosure Nothing to disclose.
Surgical and perioperative outcomes

{kind=link}
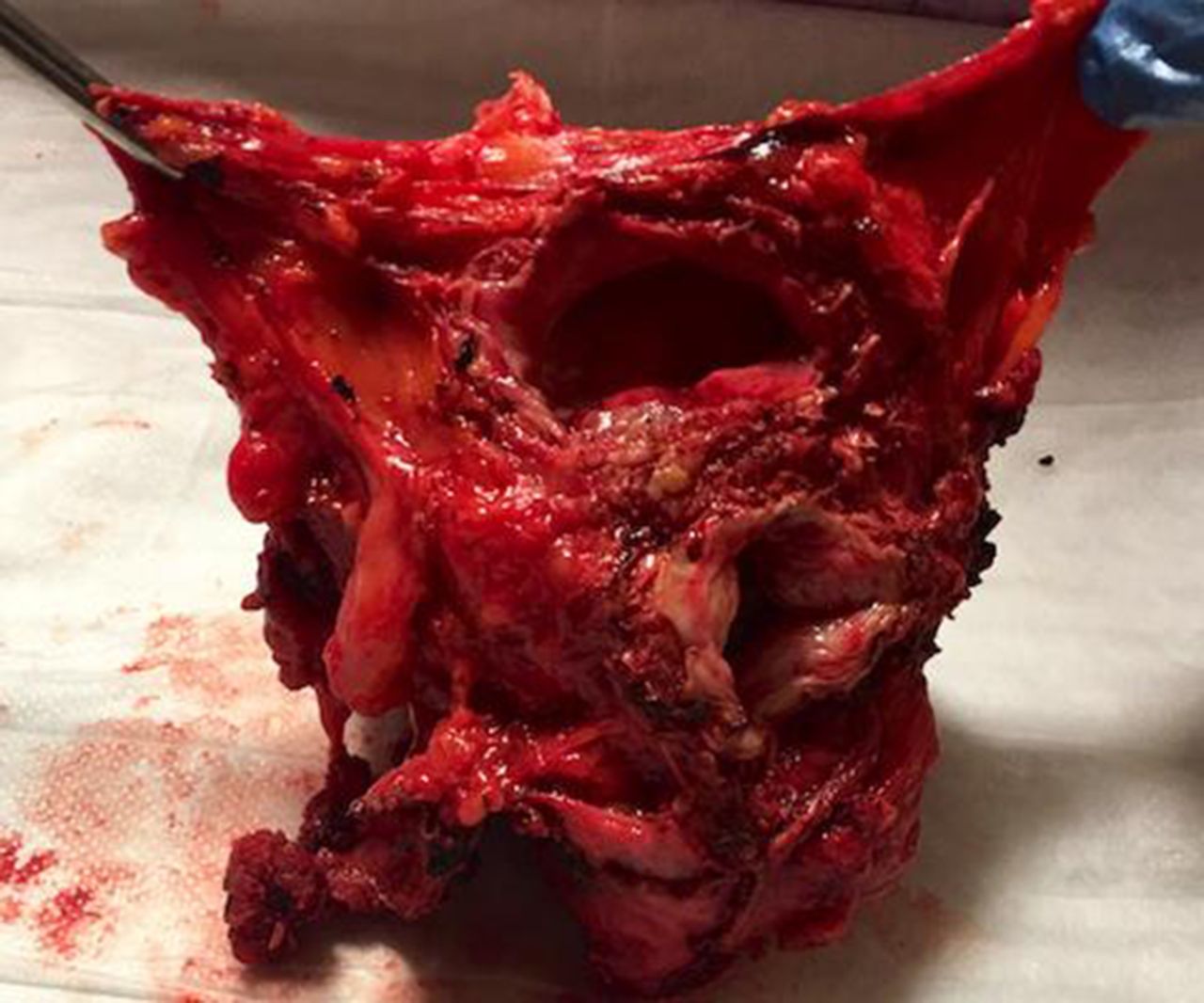
Surgical specimen of the maximum version of LM-LEER