Article Text

Abstract
Introduction/Background The aim was to evaluate the impact on survival depending on paraaortic (PA) nodes involvement and size of metastasis in locally advanced cervical cancer (LACC) after staging surgery and its safety before applying chemoradiotherapy treatment.
Methodology We conducted a retrospective study in patients with LACC (FIGO stages from IB2 to IVA) from 2000 to 2016. All patients underwent MRI imaging and a laparoscopic staging PA lymphadenectomy (LSPAL). We performed an accurate ultrastaging of positive PA nodes and classified them in two groups (node metastasis >5 mm vs ≤5 mm) in order to compare the overall survival (OS). Radiation fields were extended to the PA area only in patients with PA nodes involvement. We evaluated the morbidity and mortality of the surgery.
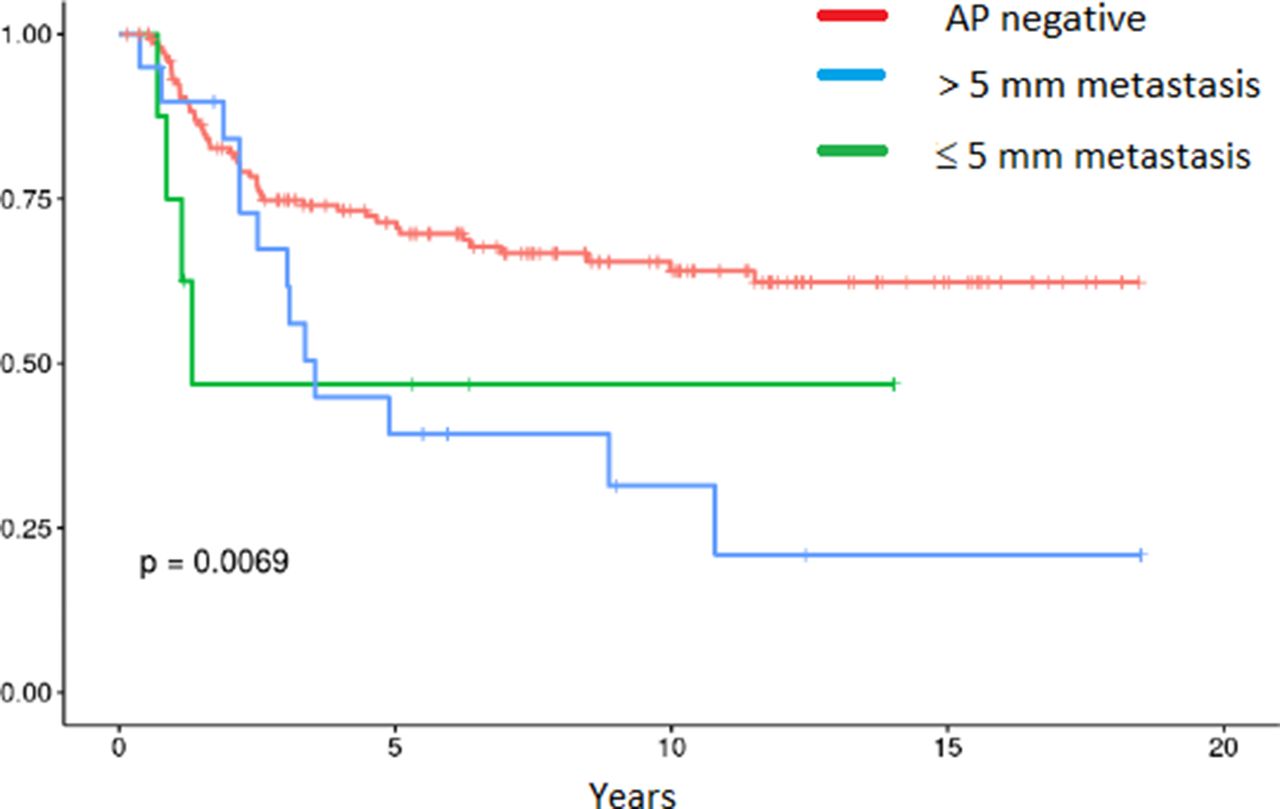
Results One hundred eighty three patients were diagnosed as a LACC. One hundred fifty patients had squamous carcinoma and thirty three patients adenocarcinoma. We observed 34 (18.5%) patients with PA nodal involvement (8 patients with PA metastasis measuring ≤5 mm and 20 measuring >5 mm). Six patients with lymph node metastasis did not have an ultrastaging study and were excluded from the analysis. Hazar Ratio for OS at 15 years were 2.51 (CI 0.90–6.98) for ≤5 mm metastasis (p 0.08) and 2.34 (CI 1.27–4.32) for >5 mm metastasis (p 0.007). Regarding surgical complications, 4 intraoperative events were reported (2,19%) although no perioperative mortality occurred. Thirteen (7.14%) early complications during the first month and 7(3.91%) late complications were reported with no mortality events.
Conclusion The size of the paraaortic lymph node metastasis in patients with LACC has prognostic implications. Overall survival in patients with negative nodes or with metastasis ≤5 mm is similar. Paraaortic lymph node staging and extended-field radiotherapy represent a survival benefit in cases with positive nodes ≤5 mm. In LACC patients LSPAL seems a safe procedure.
Disclosure Nothing to disclose.
{kind=link}
Size of the paraaortic lymph node metastasis and overall survival