Article Text

Abstract
Introduction/Background Limited data are available on the preferred policy in patients with vulvar cancer and bulky lymph nodes in the groin. Debulking of the nodes followed by radiotherapy resulted in less morbidity and similar groin control and survival compared with a complete inguino femoral groin dissection (IFL) in studies with limited patient numbers.
The aim of this study was to gather more data and confirm the ‘safety’ of debulking compared to IFL followed by radiotherapy. Historically, patients with bulky lymph nodes were treated by a complete IFL. From 2007 onwards the policy changed into nodal debulking. Groin recurrence-free survival and survival were evaluated in both groups.
Methodology Between 1982 and 2016, 217 patients were identified with positive groin lymph nodes. Clinically suspicious bulky lymph nodes and histologically confirmed as tumor positive were found in 71 patients. Before 2007, 36 patients with bulky nodes were treated by a complete IFL. After 2007, 35 patients were treated by nodal debulking. All patients received radiotherapy to both groins and pelvis. Clinical (age, tumor diameter) and pathologic (number of positive nodes, extracapsular growth) variables among the two groups were compared. Disease specific survival and groin recurrence-free survival were calculated.
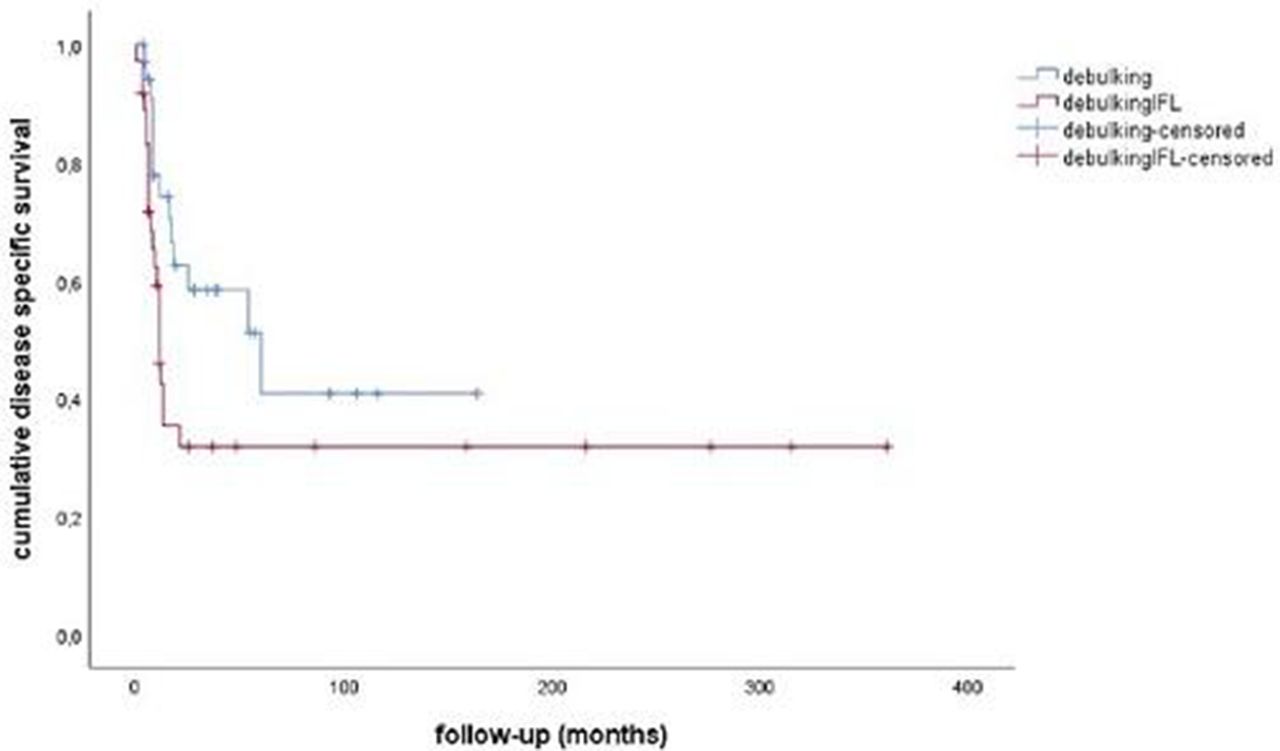
Results No difference was seen in clinical and pathological parameters between the debulking and IFL groups. Per groin analysis showed no difference in groin recurrence rate (12.3% versus 14.3%, p=0,41). The 2 year groin recurrence free survival for debulking versus IFL was 81,3% versus 73,5%, respectively (p=0.31, figure 1). Two years disease specific survival was better for patients after nodal debulking (62.5% versus 31.9%, p=0.04, figure 2).
Conclusion Because of the limited number of patients analyzed it is difficult to draw firm conclusions, but it is suggested that nodal debulking instead of formal IFL followed by radiotherapy does not compromise groin control and survival.
Disclosure Nothing to disclose.

Groin recurrence free survival for nodal debulking versus complete IFL

{kind=link}
{kind=link}
Disease specific survival for patients with nodal debulking versus complete IFL