Article Text

Abstract
Introduction/Background Following international trends for maximizing CD in EOC, we applied, in 2008, a policy for aggressive pelvic and upper abdominal surgery that included trying to remove any gross visible disease in the abdomen.
Our objective is to asses the impact of extensive procedures (Diaphragmatic resection, large and small bowel resection, complete peritonectomy, complete omentectomy, paraaortic lmph node dissection, splenectomy, resection of all visible disease) in CRS on the rate of CD, progression free (PFS), and overall survival (OS) in patients with advanced EOC.
Methodology Patients undergoing CRS between 2002–2018 were divided into group#1(2002–2008), and group#2 (2009–2018). Demographic and operative information were retrospectively reviewed.
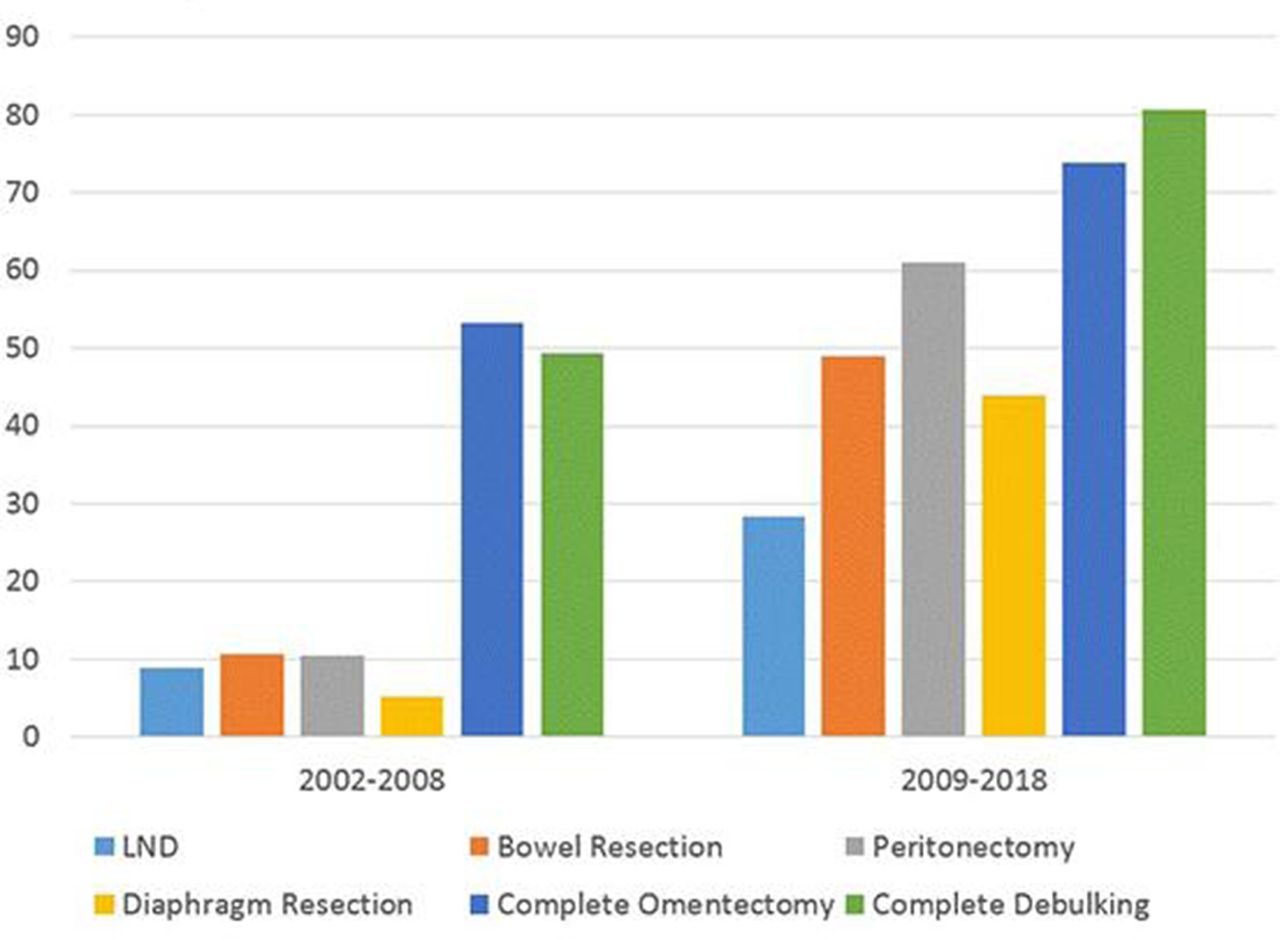
Results 204 patient with EOC (IIIC-IV) underwent CRS between 2002–2018. The number of CRS as well as performing extensive procedures (figure 1A) has significantly increased over the whole period (72 in group1 vs 132 in group2: p-value<0.001), and this coincided with a significant increase in the CD rate from 50% to 80% (p-value<0.001) (figure 1A). In stage IIIC, median PFS was significantly higher in group#2 versus group#1 (22 months, 95%CI 16.80–27.19 and 23 months, 95%CI 19.11–26.80 respectively; HR:0.965, p-value=0.036) (figure 1B). However, OS in stage IIIC was not significantly different. In stage IV, there was no statistically significant difference in PFS or OS between groups.
Conclusion Introducing extensive procedures did significantly affect the PFS in stage IIIC but not in IV. OS was not affected in both stages. The increase in number of EOC cases over the years (72 before 2009 versus 132 after 2009), which was associated with more patients with extensive tumor load and low perfomance status being admitted to our service, coupled with their shorter follow up versus patients from before 2009, may have led to the non-significant increase in OS over time.
Disclosure Nothing to disclose.
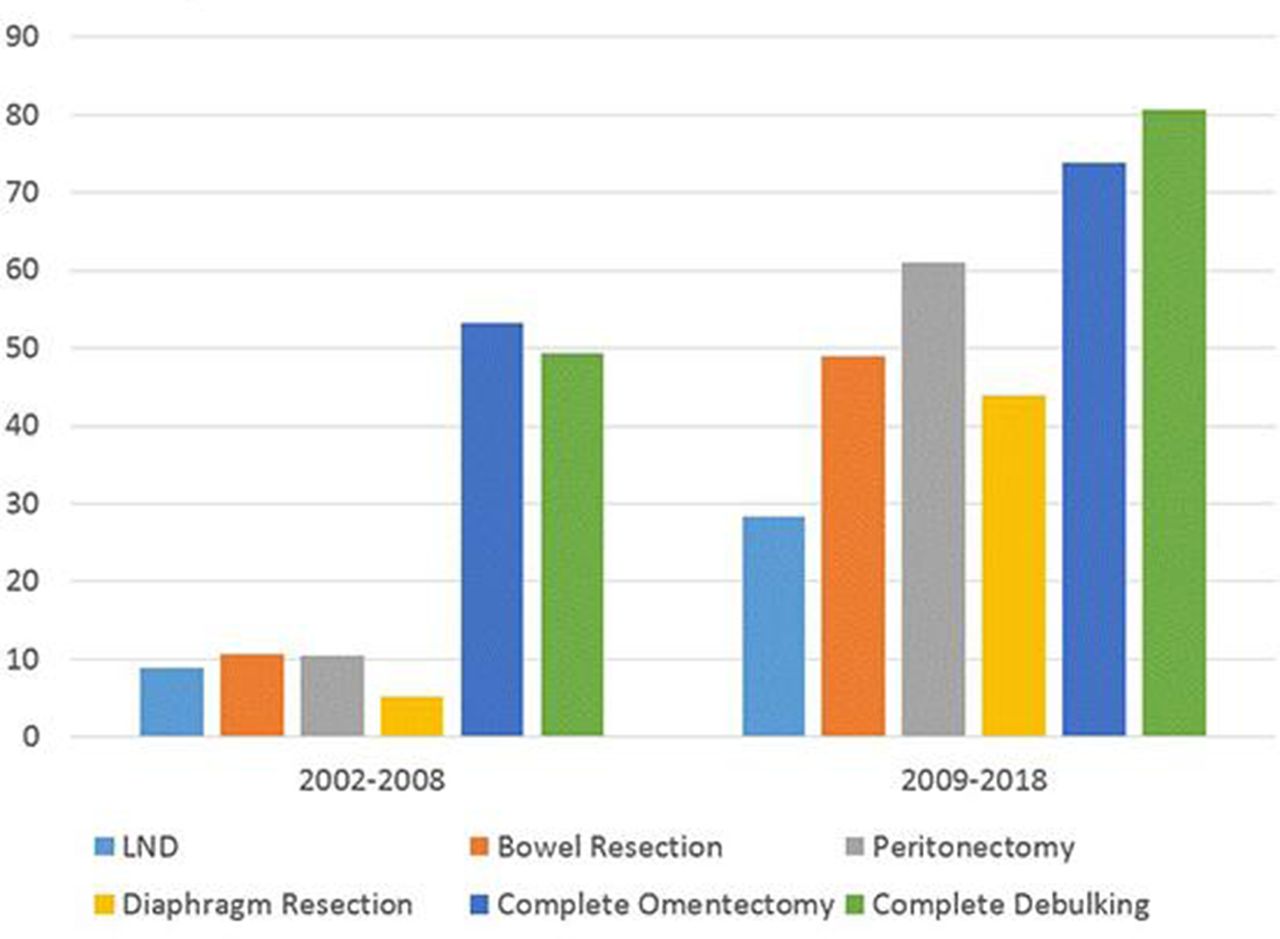
Extensive procedures and rate of CD

{kind=link}
{kind=link}
PFS in stage IIIC