Article Text

Statistics from Altmetric.com
Case presentation
A 48-year-old woman was referred to our hospital for a rapidly growing mass in the abdominal wall 3 months before presentation. The patient had no previous significant medical history. She was a non-smoker and had no relevant family history. The patient had a cesarean section delivery by a transverse suprapubic incision when she was 30 years old. The patient had a 7 year history and a clinical diagnosis of abdominal wall endometrioma. In the course of the years before presentation, the main symptomatology was localized abdominal pain in the region of the abdominal wall nodule during the menstrual cycle. When the diagnosis of endometrioma was made, a surgical excision was offered, but the patient refused. A clinical treatment was initiated with monthly medroxyprogesterone injection; however, this therapy was stopped after 3 months because of severe headaches. Subsequently, during the menstrual period, non-steroidal anti-inflammatory drugs were used, namely diclofenac or nimesulide or ibuprofen, with satisfactory pain relief. The patient had an irregular follow-up with her general gynecologist .
On presentation to our hospital, the physical examination revealed an enlarged and fixed abdominal wall mass on the cesarean section scar, measuring approximately 12 cm. The gynecological pelvic examination was unremarkable and revealed no enlarged lymph nodes. Pelvic magnetic resonance imaging (MRI) with computed tomography (CT) of the chest, abdomen, and pelvis were ordered, complemented with cancer antigen 125 (CA125) and pre-operative blood tests. Serum CA125 level was 3157.9 U/mL.
Dr Accardo de Mattos
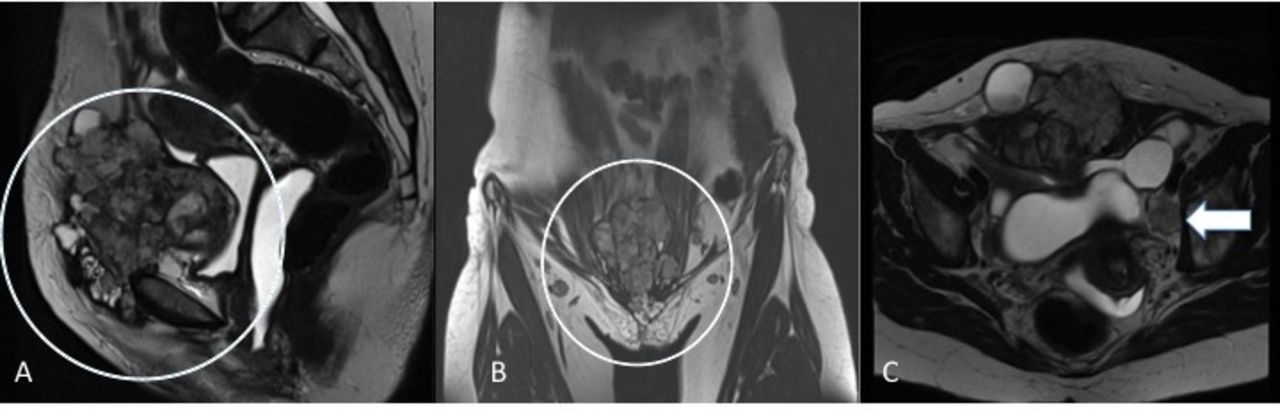
The pelvic MRI showed an infiltrative lesion measuring 10.5 × 9.0 × 8.0 cm involving the right and left anterior rectus abdominis muscle. The lesion was impinging, but not invading, the periosteum of the pubis without infiltration of either the peritoneal cavity or the bladder. In addition, there was evidence of suspicious lymph node involvement on both external iliac chains, measuring up to 1.3 cm on the right and 1.9 cm on the left (on the small axis). The right inguinal lymph nodes were slightly enlarged, measuring up to 1.2 cm . The uterus and ovaries were unremarkable. CT of the chest, abdomen, and pelvis did not show any evidence of enlarged retroperitoneal lymph nodes or other sites of suspected metastasis (Figure 1).

Pelvic magnetic resonance imaging showing a large, solid, infiltrative lesion extending from the abdominal wall, deeply infiltrating the rectus abdominis muscle and subcutaneous tissue extending into the pre-peritoneal fat. The tumor component is predominantly solid and vascularized with hematic foci. In addition, extensive iliac lymph node enlargements are noticed. (A) Sagittal plane, T2-weighted. (B) Coronal view, T2-weighted. (C) Enlarged lymph node located on the left obturator fossa with suspicious neoplastic involvement (arrow). Axial view, T2 weighted.
The patient then underwent an incisional biopsy of the abdominal wall mass. Frozen section was performed in order to achieve an adequate and representative tissue sample.
Dr Carvalho
The abdominal mass biopsy was evaluated at frozen section and showed an infiltrative neoplasia associated with fibrous tissue of scar pattern. Tumor cells were cuboidal and in complex papillary structures. The frozen section report was a malignant neoplasm potentially consistent with carcinoma or mesothelioma. The final pathology revealed a fibrous scar associated with epithelioid neoplasia with papillary growth pattern, moderate nuclear atypia, and numerous mitotic figures. Immunohistochemical study was performed to define the histological type. Calretinin, podoplanin (D2-40), and WT-1 were negative, and MOC-31 was positive, ruling out mesothelioma. Additional differential diagnoses considered were high-grade serous carcinoma and endometrioid carcinoma.
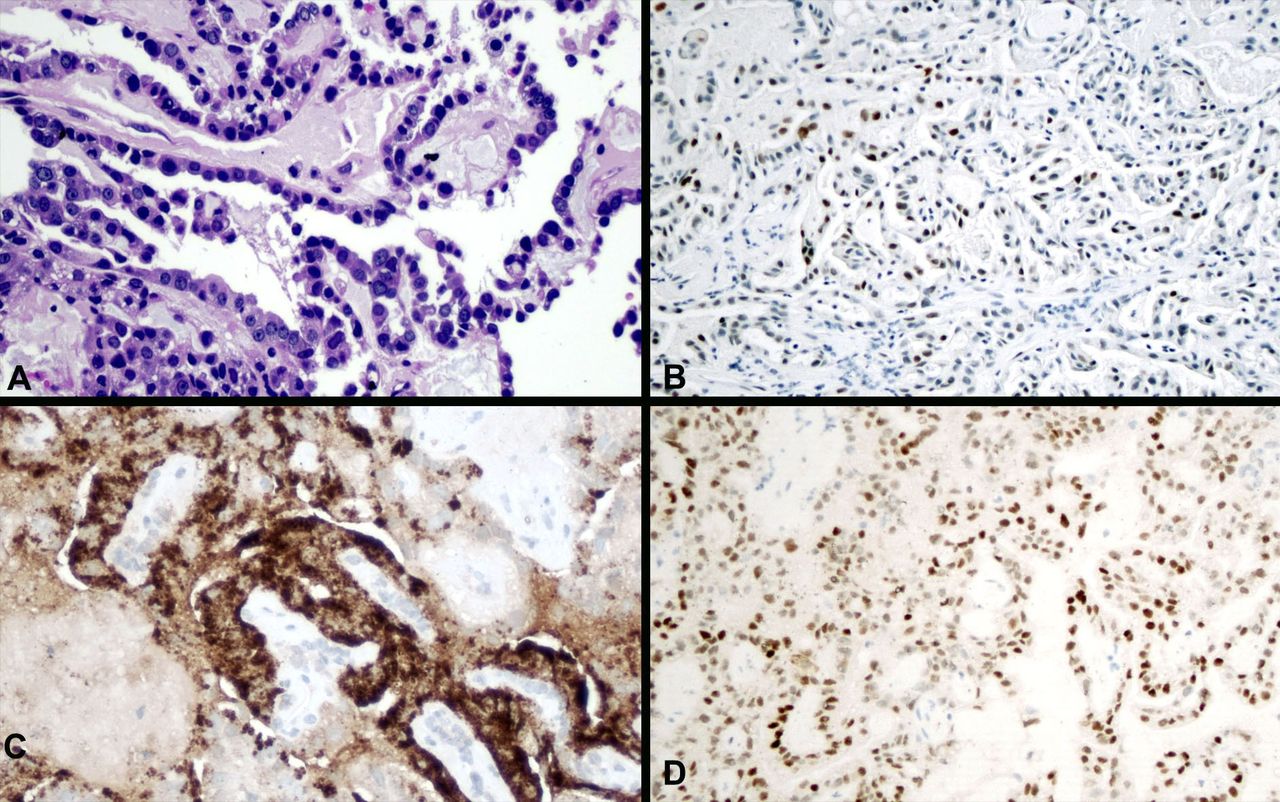
The epithelial cells were positive for PAX-8, negative for estrogen and progesterone receptors, and presented a wild-type p53 (weak expression in 40 % of tumor cells), together with non-confluent foci of p16 expression. Napsin A and hepatocyte nuclear factor 1β (HNF1β) were diffuse and strongly positive. The final diagnosis was clear cell carcinoma, most likely originating in the endometriosis (Figure 2).

Clear cell carcinoma showing (A) papillary structures with fibrovascular hyalinized cores, lined by cuboidal atypical cells with eosinophilia (hematoxylin-eosin). Immunohistochemical study revealed (B) p53 wild-type expression, (C) positive granular cytoplasmic staining for Napsin A, and (D) positive nuclear staining for hepatocyte nuclear factor-1β (HNF1β).
Dr Slomovitz
What is the natural of history of clear cell carcinoma arising in endometriosis?
Endometriosis, which is common among women of reproductive age, suggests the presence of functioning endometrial tissues outside the uterus.3 Patients with clear cell carcinoma arising in endometriosis often have a history of uterine surgery, especially cesarean section. The time between surgery and cancer diagnosis can vary widely among patients , for example, from 9 to 30 years post-uterine surgery.1–3 Scar endometriosis usually results from the intra- surgical implantation of endometrial tissues into the edge of the surgical wound in the abdominal wall’s soft tissues.2 3
Symptoms suggesting endometriosis in a surgical abdominal scar from gynecologic or obstetric surgery include a slow developing lump in or near the scar, and pain and abdominal swelling during menstruation.1 A review of 47 cases of endometriosis-associated malignant transformation in abdominal surgical scar suggests that about half of these cases have a history of endometriosis.2 However, diagnosis of clear cell carcinoma arising in endometriosis is challenging because this disease develops slowly, there is no specific marker for its malignant transformation, and it is very rare.1 The incidence of endometriosis in abdominal surgical scarring is about 0.03 % to 0.4 % , and the malignant transformation is reported in only up to 1 % of cases.1 3 Diagnosis also proves challenging due to the long time interval from original surgery ( c esarean section) until the cancer diagnosis. Many cases of clear cell carcinoma arising in endometriosis originally are diagnosed as a subcutaneous mass.
The tumor in this disease ranges widely in size, but it is usually large. In a review of 23 cases of endometriosis-associated clear cell carcinoma arising within cesarean section scars, the median diameter was 9 cm (range 2.5 –22 cm ).1
The usual outcomes, as suggested in a review of 47 cases, involve high recurrence rates and complications from extensive surgery, aggressive disease, and poor prognosis.2 Review studies also suggest a 5 year overall survival of about 40 % and a median overall survival of 42 months ( 95% CI 18.7 to 65.3 months).
What options for therapy would you discuss with this patient?
There is no standard treatment for clear cell carcinoma from endometriosis. We treat these patients as if they have metastatic uterine cancers. Most patients are primarily treated with surgery (specifically, tumor debulking and total hysterectomy, and bilateral salpingo-oophorectomy). Extensive surgery is usually needed due to the large size of the mass and the invasive nature of the disease at diagnosis.
Because it is considered metastatic disease, I would reserve pelvic lymph node dissection to those patients who have grossly enlarged lymph nodes. Also, patients with limited disease may benefit from pelvic lymph node dissection to help determine the best treatment options. In addition, many of these tumors may be responsive to hormone therapy and patients may benefit from estrogen blockade.
The patient underwent abdominal wall tumor resection, including resection of the inferior portion of the rectus abdominis muscle until its insertion in the pubis with en-bloc superficial inguinal lymphadenectomy. Aiming at complete resection of the tumor and cesarean section scar, a transverse suprapubic incision was made, followed by a second infra-umbilical transverse incision, planned to facilitate the abdominal wall reconstruction. It was required to resect the inferior third of the rectus abdominis muscle and its tendon, jointly with the periosteum of the pubic bone. A smaller portion of the transversus abdominis, internal and external oblique were also included, on the left and right sides. The superficial inguinal lymphadenectomy was performed contiguously with the specimen resection, bilaterally. The peritoneum of the abdominal cavity was intact and without implants. Its removal was necessary due to adhesions to the tumor mass. The abdominal wall resection was followed by a subcutaneous detachment from the aponeurosis, which was incised in the midline. Additionally, a type A hysterectomy with adnexectomy followed by systematic pelvic and para-aortic lymphadenectomy with radical omentectomy were performed. The lymphadenectomy was performed given that bulky lymph nodes were noticed on the external iliac and obturator fossa chains bilaterally. The abdominal wall reconstruction was performed with a special mesh (Symbotex composite mesh – Medtronic) specifically designed to prevent adhesions of the abdominal viscera, superimposed by a polypropylene mesh (Figure 3).

Stepwise photographs illustrating the resection and reconstruction of the abdominal wall. (A) Pre-operative: delimited resection area and planned incisions aiming at macroscopic free margins and abdominal wall reconstruction. (B) Incision on the skin, including the cesarean section scar on the specimen. (C) Final aspect after ressection of the abdominal wall tumor. (D) Abdominal wall suture and insertion of a mesh to prevent abdominal adhesions. (E) Superimposed polypropylene mesh for reinforcement of the abdominal wall. (F) Final aspect after reconstruction.
The total operating time was 525 min; of these, 300 min were required for the resection procedures and 225 min for the reconstruction. There were no intra-operative complications. The estimated blood loss was 500 mL and 2 units (600 mL) of red blood cells were transfused. The patient was in the intensive care unit for 1 day. The post-operative course was uneventful and the patient was discharged on post-operative day 4 without complications.
Dr Slomovitz
At the time of surgery, would you have performed hysterectomy and lymphadenectomy or only resection of the mass? Please, also comment on the role of lymphadenectomy
I would have performed hysterectomy, bilateral salpingo-oophorectomy, and lymphadenectomy. Even though the patient ’s pelvic MRI suggested that the uterus and ovaries were unremarkable, a hysterectomy would have been warranted due to the final pathological diagnosis originating in the endometriosis. In terms of justification for performing a lymphadenectomy, the patient ’s pelvic MRI showed extensive lymph node enlargements (Figure 1), specifically potential lymph node involvement on both external iliac chains up to 1.3 cm on the right and 1.9 cm on the left. Imaging also showed up to a 1.2 cm enlargement of the right inguinal lymph node. However, CT chest/abdomen/pelvis suggested no evidence of enlarged retroperitoneal lymph nodes or other metastasis. Lymphadenectomy here is mainly performed as part of a debulking procedure.
Dr Carvalho
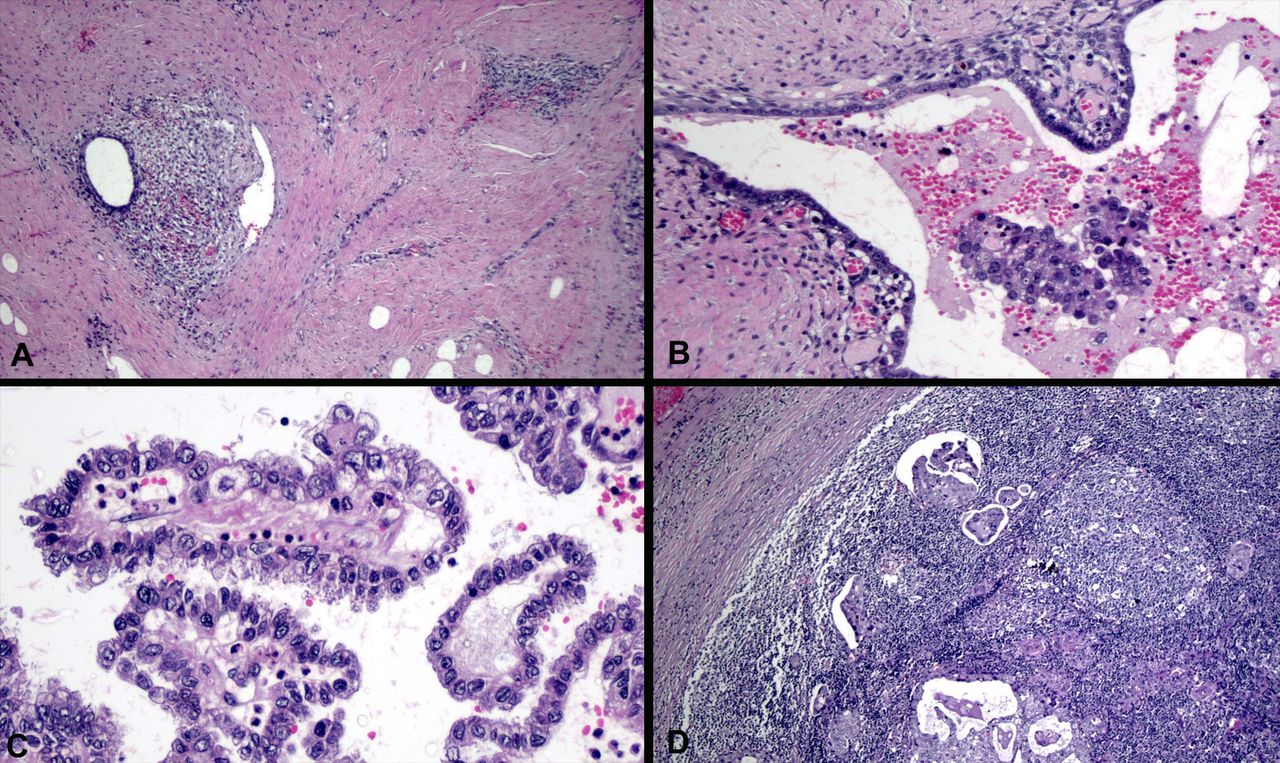
The surgical specimen corresponding to tumor excision measured 25.0 × 12.0 × 11.5 cm and revealed a tumor measuring 10.0 cm in the largest axis located in the abdominal wall, between the skin and the rectus abdominis muscle. Microscopic examination showed a clear cell carcinoma with similar characteristics to the previous biopsy; however, the surgical specimen revealed a higher degree of atypia and this was associated with endometriosis. The lesion was localized mainly in the adipose plane with infiltration of superficial skeletal muscle bundles of the deep plane and extension through the recent scar of a previous biopsy in the suprajacent dermis. The tumor was associated with areas of stroma and glands of endometriosis foci. No vascular or neural infiltration was seen. Surgical margins were negative for disease. A total of 83 lymph nodes were examined ( nine inguinal, 30 para-aortic, 24 left pelvic, and 20 right pelvic). Metastatic disease was identified in five lymph nodes; two were in the inguinal nodes, two were right pelvic, and one left pelvic. The largest metastasis was present in a left pelvic lymph node and measured 46.0 mm . One of the inguinal metastases presented an extra-capsular extension. The remaining lymph nodes only had evidence of micrometastases. Bilateral adnexal, uterus, and omentum were negative for any disease. Endometriosis was also identified on the surface of the left ovary (stromal endometrioid tissue with hemorrhage) and in tubal fimbria (endometrioid stroma with diffuse smooth muscle metaplasia) (Figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Post-operative pathology. (A) Fibrous scar with multiple endometriosis foci composed of endometrioid stroma and glands. (B) Glandular space of endometriosis partially surrounded by endometrioid stroma and showing tumor cells in the lumen. (C) Detail of clear cell carcinoma with papillar structures lined by atypical clear and eosinophilic cells. (D) Inguinal lymph node with metastasis.
Dr Slomovitz
What is the role of adjuvant therapy in this patient? Please comment on both adjuvant chemotherapy, radiotherapy, or both
Even though the effect on the overall survival rate or progression-free survival of adjuvant chemotherapy or radiotherapy remains unclear, I would encourage adjuvant treatment. Case reviews usually describe using platinum-based chemotherapy ± - l ocal radiation for adjuvant treatment.3
The recommendation was made for the patient to undergo systemic adjuvant therapy in the form of six cycles of carboplatin and paclitaxel. Immediately before the adjuvant treatment, the serum CA125 level was 11.8 U/mL. To date, the patient is undergoing the fourth cycle of chemotherapy without evidence of disease.
Dr Slomovitz
Closing summary
This is a very interesting case. I commend the primary medical team for their care. Fortunately, these are rare tumors that we do not have to often deal with. In summary, endometriosis that involves the skin occurs in only 0.5 – 1 % of patients with that disease.4 Clear cell carcinoma arising in an abdominal scar is a tumor generally arising in young women and is an aggressive disease with poor prognosis, and a 5 year survival of approximately 40 % . It often arises in a cesarean section scar or from prior abdominal surgeries. Routine imaging is not specifically helpful in detecting malignancy and there are no specific markers for it. Usually at the time of diagnosis these tumors can be quite large. Radical excision is usually performed, with or without adjuvant therapy. Treatment of abdominal wall defects can often pose a challenge and abdominal hernias may be common, with a prevalence ranging from 12 – 50 %.5 Synthetic implant mesh is frequently used with or without skin grafts. In the event that synthetic mesh implants cannot be used, one may opt for musculocutaneous flaps with rectus femoris or fasciocutaneous flaps from the anterolateral thigh.6 Regarding disease-free survival, there seems to be a worse trend towards clear cell carcinoma when compared with endometrioid carcinoma. Optimal resection, adjuvant chemotherapy, and possibly radiation are most likely the best treatment options for these patients . Hormonal therapy has been proposed in non-operable cases with progestins, but the benefits are not clear.
Footnotes
Contributors All authors contributed equally to the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval This study was approved by the research ethics committees of Instituto Brasileiro de Controle do Câncer (reference No 3.380.605).
Provenance and peer review Commissioned; internally peer reviewed.