Article Text

Abstract
Introduction BRCA gene mutations are associated with hereditary ovarian cancer. BRCA plays a key role in genome integrity, and mutations result in an increased risk for ovarian cancer. Although various guidelines recommend BRCA testing in patients with ovarian cancer, data on germline BRCA (gB RCA) mutation frequency in ovarian cancer in Japan are scarce.
Objective This study aimed to determine gBRCA1/2 mutations in Japanese patients with ovarian cancer, stratified by clinicopathological characteristics, and to assess patients’ satisfaction with pre-test genetic counseling.
Methods The CHARLOTTE study (CHARacterizing the cross-sectionaL approach to Ovarian cancer: geneTic TEsting of BRCA; UMIN000025597) is the first large multicenter epidemiological survey of Japanese women, aged ≥20, with newly diagnosed ovarian cancer (epithelial, primary peritoneal, or fallopian tube cancer), with histologically confirmed specimens. Patients were enrolled sequentially and underwent pre-test genetic counseling for BRCA testing. Blood samples were centrally tested for the presence or absence of known gBRCA mutations. A questionnaire was used to assess patient satisfaction with pre-test genetic counseling.
Results A total of 634 patients with a mean age of 56.9 years were included. Most patients (84.2%) had epithelial ovarian cancer, and 51.1% had FIGO stage III–IV cancer. Nearly all patients (99.5%) received genetic counseling before the BRCA testing, either by an obstetrician-gynecologist (42.0%) or a clinical geneticist (42.0%). The overall prevalence of gBRCA1/2 mutations was 14.7% (93/634), with gBRCA1 mutations (9.9%) more common than gBRCA2 mutations (4.7%). High-grade serous carcinoma showed a prevalence of gBRCA mutations of 28.5%. Most patients were satisfied with pre-test counseling, irrespective of the service provider’s professional position.
Discussion Patients with high-grade serous carcinoma and family history of ovarian cancer had a slightly higher prevalence of gBRCA mutations, but none of the subgroups had considerably high gBRCA mutation prevalence. These data suggest that gBRCA testing should be carried out in all patients with ovarian cancer.
- cross-sectional study
- genetic testing
- ovarian cancer
- BRCA
- japanese
This is an Open Access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
HIGHLIGHTS
The overall prevalence of germline BRCA1/2 mutations was 14.7% in Japanese patients with ovarian cancer.
Our data suggest that germline BRCA testing should be carried out in all patients with ovarian cancer.
Most patients were satisfied with pre-test counseling, irrespective of the provider's profession.
Introduction
Among breast and ovarian cancers, between 5% and 10% are hereditary.1–3 These hereditary cancers are associated with mutations in the BRCA1 or BRCA2 genes, which are germline breast cancer susceptibility genes with autosomal dominant inheritance.3 4 Functional BRCA1 and BRCA2 proteins are present in normal breast and ovarian tissue and are involved in homologous recombination mediated DNA repair with wide-ranging functions in cells, and play a key role in genome integrity.5–7 Mutations that interfere with the critical BRCA function lead to increased susceptibility and progression of breast and ovarian cancers.7
BRCA is a biomarker with clinical significance and has implications for therapy outcomes, drug susceptibility (including that to platinum agents), and prognosis.7–11 Various guidelines worldwide, including National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology and the American College of Obstetricians and Gynecologists Guidelines, recommend testing for germline BRCA (gBRCA) mutations in patients with ovarian cancer.12 13
Data on the frequency of gBRCA1 and gBRCA2 mutations in Japanese patients with ovarian cancer are scarce, largely because of the lack of financial coverage for BRCA genetic testing by the National Health Insurance system. Research data are also limited in Japan; a few studies have been published, but no nationwide large-scale study has been conducted. Sekine et al reported that 45 of 82 Japanese families with a history of ovarian cancer had gBRCA1/2 mutations.14 Hirasawa et al reported that among 230 patients with ovarian, fallopian tube, or peritoneal cancer, only 27 patients (11.7%) had gBRCA1/2 mutations.4
This study, CHARLOTTE (CHARacterizing the cross-sectionaL approach to Ovarian cancer: geneTic TEsting of BRCA), was the first multicenter epidemiological survey conducted to investigate gBRCA1/2 mutations in Japanese patients with ovarian cancer. The primary objective was to examine the frequency of gBRCA1/2 mutations in patients with newly diagnosed ovarian cancer. As pre-test explanation and proper genetic counseling are important aspects of patient care, we evaluated patient understanding and satisfaction with this counseling.
Methods
Study design
This was a collaborative multicenter, large-scale, cross-sectional study conducted across 63 eligible institutions that provided a pre-test genetic counseling service, in all regions of Japan. Study registration occurred between December 2016 and June 2018.
Ethical approval was obtained from the institutional review boards of all participating institutions. The study was conducted in accordance with the principles of the Helsinki Declaration. All patients provided written informed consent to participate in the study and approved the submission and analysis of histopathological specimens. All patient data were anonymized by the investigator. This study was registered at the University hospital Medical Information Network (UMIN) Clinical Trials Registry (UMIN000025597).
Patients
Eligible patients were registered in serial order (to avoid selection bias) by the respective attending physicians throughout the study period. The inclusion criteria were as follows: Japanese women aged ≥20 years, newly diagnosed with ovarian cancer, with histologically confirmed diagnosis, based on surgically resected specimens, and with histological specimens evaluated by central pathological review. Patients were excluded if they had an acute or chronic disease, a mental illness that could affect the study results as determined by their physician, or if their participation in the study was judged to be inappropriate by their physician. Patients were also excluded based on the centrally assessed histological classification of the surgically resected specimen.
Data sources and measurements
Patients’ medical charts were reviewed for demographic data, medical history, and information about ovarian cancer. Family history of cancer was obtained during pre-test genetic counseling at the first visit. Data collected included patient demographic and clinical characteristics (date of birth, age), medical history, medications, menopausal status, obstetric history, and blood biochemical testing (cancer antigen 125). Data were also collected regarding ovarian cancer, including date of diagnosis, pathological and histological type, and grade on diagnosis and International Federation of Gynecology and Obstetrics (FIGO) classification. Blood samples from all eligible patients were collected in 10 mL ethylenediaminetetraacetic acid tubes and centrally tested for the presence or absence of known gBRCA mutations (gBRCA1 and gBRCA2) by Myriad Genetics, Inc (Salt Lake City, Utah, USA).
Confirmation of the histological diagnosis was performed centrally by a pathologist assigned by the Japanese Gynecologic Oncology Group using hematoxylin and eosin slide specimens from tumor tissues. The central histological evaluation and diagnosis of ovarian cancer was based on the WHO classification of tumors of female reproductive organs.15
All patients underwent pre-test genetic counseling, which was provided by a trained obstetrician-gynecologist or oncologist, clinical geneticist, or certified genetic counselor. If the test was positive or indicated a variant of uncertain significance, the patient received further genetic counseling. A genetic specialist revised the document used to provide counseling for gBRCA testing.
To assess patient satisfaction with the pre-test explanation of gBRCA testing, a written questionnaire, including eight questions, was administered to all patients after receiving the pre-test counseling, but before they received their results. Responses were given on a scale of 1 to 5, with 5 indicating the highest satisfaction. Questionnaires were sent to CMIC Healthcare Co, Ltd (Tokyo, Japan), in a pre-specified reply envelope.
Study endpoints
The primary endpoint of the study was the prevalence of gBRCA1/2 mutations in patients with newly diagnosed ovarian cancer in Japan. A positive BRCA mutation was defined as a deleterious or suspected deleterious mutation.
Secondary endpoints were the prevalence of gBRCA1/2 mutations in subgroups stratified by histological classification, FIGO stage, and family history of cancer, and the evaluation of patient satisfaction with pre-test genetic counseling.
Statistical methods
Details of the sample size calculation are given in online supplementary text 1, supplemental digital content 2. Descriptive statistics were used for baseline demographic and clinical characteristics, with n (%) for categorical variables and mean±SD for continuous variables. The full analysis set consisted of all patients who underwent gBRCA mutation testing and had histological specimens available for central pathology confirmation.
Supplemental material
The prevalence of gBRCA1/2 mutations was calculated, together with 95% CIs, for all patients, and was stratified by patient background factors, diagnosis, histological classification, staging presence, or absence of family history of cancer in close relatives, and by type of cancer in the family history. All statistical analyses were performed using statistical analysis software (SAS) 9.4 (SAS Institute, Cary, North Carolina, USA).
Results
Patients
Patient disposition is shown in online supplementary figure 1, supplemental digital content 1. A total of 666 patients were enrolled, but three patients withdrew and 29 were excluded from the full analysis set, based on centralized pathological results. A total of 634 patients were thus included in the final analysis.
Supplemental material
Patient characteristics are described in online supplementary table 1, supplemental digital content 2. Patients in the full analysis had a mean age of 56.9 years; 72.9% of patients were postmenopausal. Epithelial ovarian cancer was the most common diagnosis (84.2%), 48.4% of the ovarian cancers were FIGO stage I–II, and 51.1% were FIGO stage III–IV.
Primary outcomes
The overall prevalence of gBRCA1/2 mutations in the study population was 14.7% (93/634) (Figure 1). The prevalence of gBRCA1 mutations (9.9%) was higher than that of gBRCA2 mutations (4.7%). Test results for 29 (4.6%) patients were variants of uncertain significance. No patients had both gBRCA1 and gBRCA2 mutations.
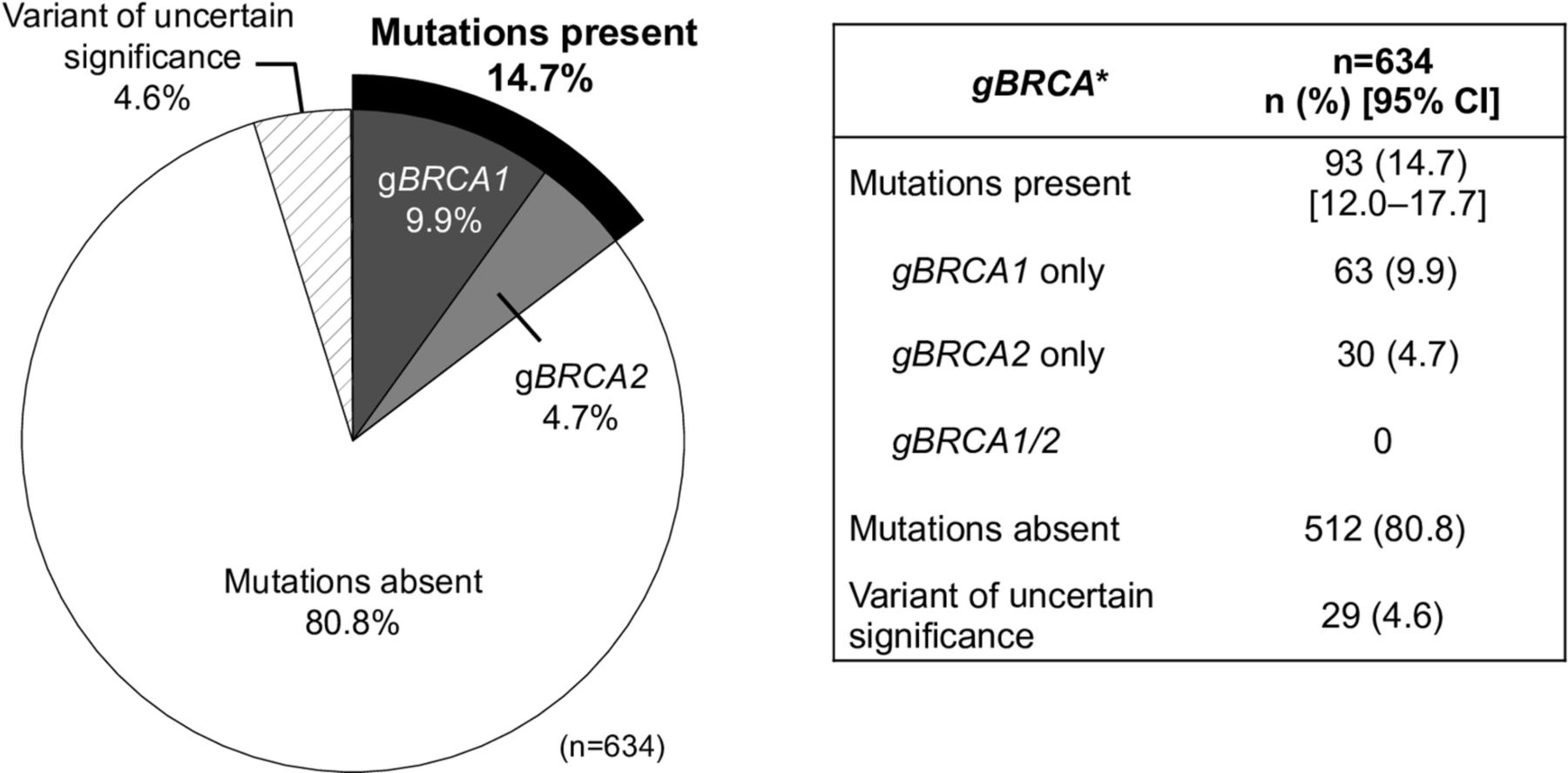
Prevalence of gBRCA1/2 mutations. *gBRCA mutations were interpreted using the Myriad Database. CI, confidence interval; gBRCA, germline BRCA.
Secondary outcomes
Overall, stratification by patient background factors did not disclose any subgroup with a considerably high prevalence of gBRCA mutations, except for those with a family history of cancers (Table 1 and Figures 2A and 2B). The prevalence of gBRCA mutations was 9.8% in patients under 41 years of age and 15.0% in those over 41 years of age. Patients under 40 years old with gBRCA mutations comprised 0.5% of the study population (see online supplementary figure 2, supplemental digital content 1, which shows the prevalence of gBRCA mutations in the study population by age). No notable trend was observed in the prevalence of gBRCA mutations according to menopausal status.
The prevalence of gBRCA mutations was highest in fallopian tube carcinoma (29.2%) and lowest in epithelial ovarian cancer (12.7%) (see online supplementary figure 3, supplemental digital content 1, which shows the prevalence of gBRCA mutations by cancer diagnosis). For epithelial ovarian and primary peritoneal cancers, the prevalence of gBRCA1 mutations was higher than that of gBRCA2, whereas for fallopian tube carcinomas, the prevalence of both gBRCA1 and gBRCA2 mutations was the same at 14.6% (online supplementary figure 3, supplemental digital content 1). The age distribution for epithelial ovarian cancer, primary peritoneal cancer, and fallopian tube cancer is shown in online supplementary figure 4, supplemental digital content 1. Patients with epithelial ovarian cancer, primary peritoneal cancer, and fallopian tube cancer were diagnosed as FIGO stage IV in 11.4%, 25.0%, and 12.5% of cases, respectively (online supplementary figure 5, supplemental digital content 1, which shows FIGO stage distribution by carcinoma type). The prevalence of gBRCA1/2 mutations by histological type is presented in Table 1. In patients with high-grade serous carcinoma the prevalence of gBRCA1/2 mutations was 28.5%, followed by low-grade serous carcinoma which had a prevalence of 20.0%. In endometrioid and clear-cell types the prevalence was 6.7% and 2.1%, respectively, while in mucinous ovarian cancer the prevalence was 0.0%.
Prevalence of germline B RCA1/2 (gBRCA1/2) mutation classified by patient background and ovarian factors
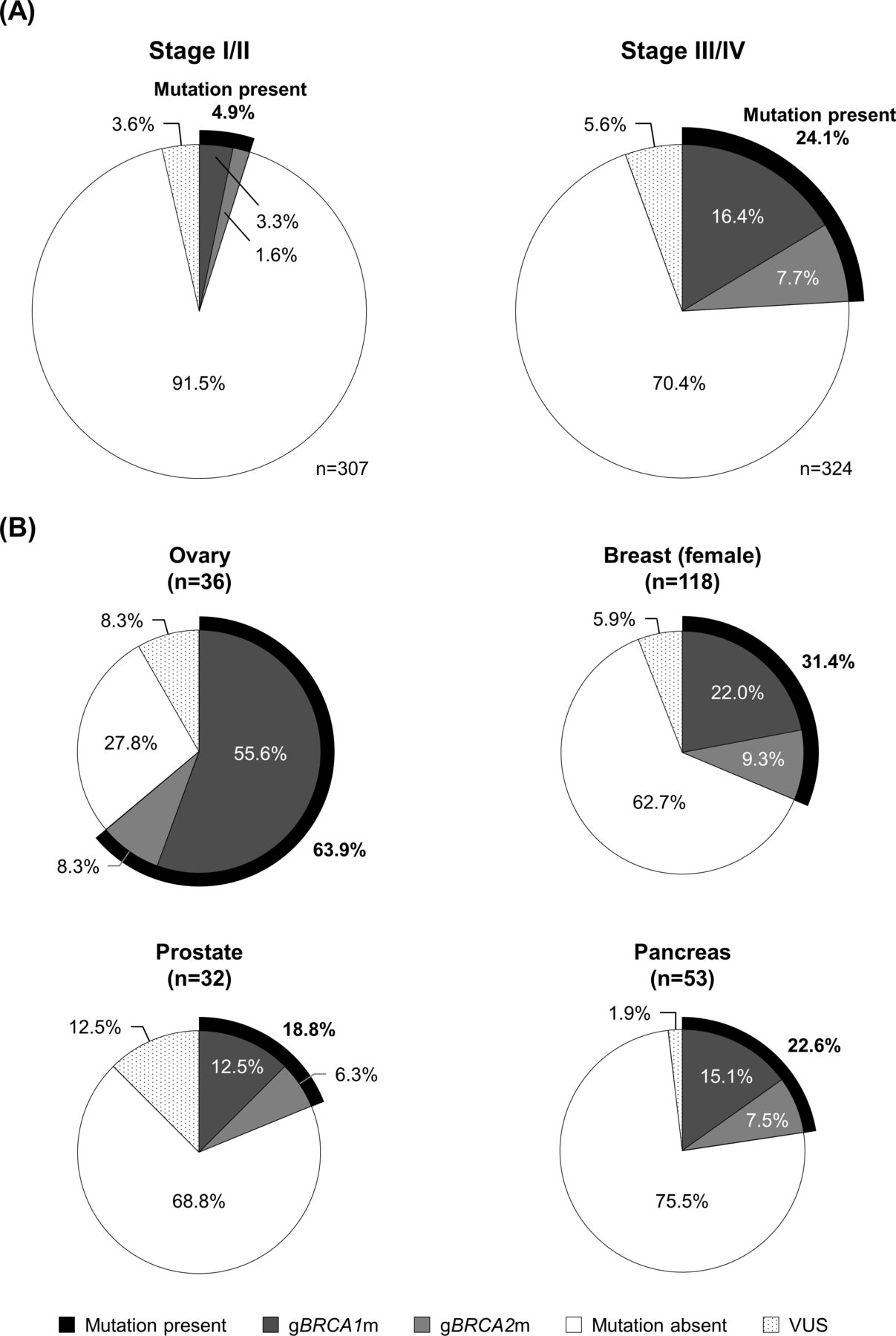
FIGO stages showed a general increasing pattern in the prevalence of gBRCA mutations. The prevalence of gBRCA mutations in patients diagnosed with FIGO stage I was 3.4% compared with 20.0% in those with FIGO IV (Table 1). When grouped into stage I–II and stage III–IV, the prevalence of gBRCA mutations was 4.9% and 24.1%, respectively (Figure 2A). High-grade serous ovarian cancer accounted for 69.8% of those diagnosed with FIGO III or IV and 14.7% of those with stage I or II (online supplementary figure 6, supplemental digital content 1, which shows cancer histological sub-types by FIGO stage). The prevalence of gBRCA mutation in high-grade serous cancers was generally high compared with other histological types. Further, gBRCA mutation was also observed in patients with early-stage non-serous ovarian cancer (Figure 3). None of the patients with mucinous cancers had gBRCA mutation (Table 1).

Prevalence of gBRCA1/2 mutations stratified by (A) FIGO stage, and (B) family history of cancer. In panel (A), three patients with a FIGO stage of ‘other’ were not included in the analysis. FIGO, International Federation of Gynecology and Obstetrics; gBRCA, germline BRCA.

{kind=link}
{kind=link}
{kind=link}
Prevalence of gBRCA mutation by histological sub-type and FIGO stage. Three patients with a FIGO stage of ‘other’ were not included in the analysis. FIGO, International Federation of Gynecology and Obstetrics; gBRCA, germline BRCA.
When cancer history in first- or second-degree relatives was grouped by type of BRCA-related cancer, the prevalence of gBRCA mutations was highest for patients with a family history of ovarian cancer (63.9%) and breast cancer (31.4%) (see Figure 2B and supplementary table 2, supplemental digital content 2, which shows relatives’ cancer sites and prevalence of patient BRCA mutations).
During the informed consent process, 99.5% of patients received pre-test genetic counseling (Table 2). Most of the pre-test genetic counseling was provided by either an obstetrician-gynecologist (42.0%) or a clinical geneticist (42.0%). Follow-up genetic counseling was provided in 91.8% of the 122 patients with a positive or variant of uncertain significance BRCA test result, which in most cases (80.4%) was done by a clinical geneticist. Twenty-two (3.5%) patients were not notified of the results of genetic testing. Reasons for non-notification included disclosure not wanted (13 patients), death of patient (four patients), transferred to a different hospital or difficulty in visiting the hospital (three patients), or notification scheduled after database lock (two patients).
Provision of genetic counseling
The level of patient satisfaction with pre-test genetic counseling and their level of satisfaction depending on the provider was high overall (see online supplementary table 3, supplemental digital content 2). For each question, irrespective of the provider, over 96% provided satisfaction.
Discussion
The CHARLOTTE study is the first multicenter, epidemiological, prospective survey to investigate the frequency of gBRCA1/2 mutations among Japanese patients with newly diagnosed ovarian cancer, focusing on relevant sub-populations. Current findings show that the overall prevalence of gBRCA1/2 mutations in the sample population was 14.7%, with a higher prevalence of gBRCA1 than gBRCA2. When categorized by patient factors, no subgroup had a considerably higher prevalence of gBRCA mutations.
The gBRCA1/2 mutation prevalence found in this study is consistent with that previously reported in Japan and other countries. Hirasawa et al conducted a single-center study and reported a gBRCA mutation prevalence of 11.7%.4 International studies also reported similar findings; 13.8% in a European and US multicenter study and 12.1% in a Taiwanese study.16 17 Ovarian cancer includes hereditary breast and ovarian cancers at a similar rate regardless of race or ethnicity; a consideration important to bear in mind when conducting medical examinations.
The prevalence of gBRCA mutations varied by histology (mucinous, clear-cell, endometrioid, low-grade serous, and high-grade serous carcinoma: 0%, 2.1%, 6.7%, 20.0%, and 28.5%, respectively). The ratio of histologic types differs between Japan, Europe, and North America, with a lower prevalence of high-grade serous carcinoma in Japanese populations than in Caucasians, which might have affected the prevalence of gBRCA mutations.18 However, we should note that in the present study the prevalence of gBRCA1/2 mutations in patients with high-grade serous carcinoma was slightly higher (28.5%) than that reported in previous studies.8 19 Alsop et al (Australia) reported a gBRCA mutation prevalence of 17.1% in patients with high-grade serous carcinoma, and Norquist et al (USA) found a combined gBRCA1 and gBRCA2 prevalence of 16.0%.8 19 Nonetheless, the results of our study are consistent with a recent study in Japan that reported a gBRCA prevalence of 29.7% in patients with high-grade serous carcinoma.4 In this study, patients with mucinous cancers did not have gBRCA mutations, which is consistent with the statement of the NCCN guidelines.12 The prevalence of gBRCA mutations generally increased with increasing FIGO stage; the prevalence was higher among high-grade, FIGO stage III–IV serous ovarian cancers than stage I–II cancers. Additionally, there was a generally higher prevalence of gBRCA mutations in high-grade serous carcinoma than in other histological types. Thus, the increasing prevalence of gBRCA mutations in FIGO III–IV cancers correlated with the prevalence of high-grade serous ovarian cancer. In both serous and non-serous ovarian cancers, gBRCA mutations were noted in the earlier disease stages. Therefore, it is difficult to speculate about the presence of gBRCA mutations according to the histological types and stages, and we consider that gBRCA testing should be conducted at all stages of ovarian cancer.
Mutations in the BRCA genes can also occur without a positive family history of BRCA-related cancers. In this study, a family history of cancer was associated with a slightly higher prevalence of gBRCA mutations. The prevalence of gBRCA mutations was highest with a family history of ovarian (63.9%) or breast cancer (31.4%). These findings are consistent with the results of other studies, with a higher prevalence in those with a family history of ovarian cancer.4 8 20 21 Lee et al also reported a higher standardized incidence ratio of ovarian cancer in all first-degree relatives of patients with ovarian cancer (2.5, 95% CI 1.6 to 4.0) compared with the standardized incidence ratio of ovarian cancer in all first-degree relatives of patients with breast cancer (1.0, 95% CI 0.7 to 1.4).22 Nonetheless, a gBRCA prevalence of 7.4% was observed in patients without a family history (first- or second-degree relatives) of cancer in our study. Overall, our results suggest that genetic testing is warranted for all patients with ovarian cancer, regardless of family history or cancer risk factors, which is in line with NCCN guidelines.12 Results of genetic testing will encourage other family members to consider undergoing the same testing before the onset of ovarian cancer and allow for regular check-ups and prophylactic removal for risk reduction.23 24
Genetic counseling before genetic testing is necessary to promote the correct understanding of results and genetic risk of cancer among family members. The proportion of patients satisfied with pre-test genetic counseling was high (>96%), irrespective of who provided the gBRCA test information. These results indicate that trained clinicians, cancer specialists, and other health professionals can effectively conduct pre-test genetic counseling in a dedicated setting.25 Given that the pre-test genetic counseling framework is undergoing further development in Japan, the best option might be to provide genetic counseling through multidisciplinary collaboration among different healthcare professionals.
These findings were based on Japanese clinical practices, and their application may be limited in other countries with different clinical practices. The varying number of patients included from different sites (online supplementary table 4, supplemental digital content 2) was another limitation; no upper limit was set for the registration of patients at individual sites, and only a few patients were registered at some sites.
Conclusions
The overall prevalence of gBRCA1/2 mutations in patients with ovarian cancer was 14.7%, with a higher prevalence of gBRCA1 than of gBRCA2. While high-grade serous carcinoma and family history, particularly of ovarian cancer, showed a somewhat higher prevalence of gBRCA mutations, none of the subgroups had considerably high gBRCA mutation prevalence overall. These findings indicate that gBRCA testing should be performed in all patients with ovarian cancer. Most patients were satisfied with the pre-test counseling provided, irrespective of the professional position of the service provider.
Acknowledgments
We thank Dr Masami Arai (genetic testing), Dr Yuko Sasajima, Dr Reiko Watanabe (Central Pathological Diagnosis Committee members), and the non-profit organization Japanese Gynecologic Oncology Group. We thank Dr Ingrid de Ruiter, MD, PhD, of Edanz Medical Writing for providing medical writing support, which was funded by AstraZeneca K.K. in accordance with Good Publication Practice guidelines (http://www.ismpp.org/gpp3).
References
Footnotes
Contributors TE, DA, YW, JK, NT, TS, and HT conceived and designed the study. KH was involved in data acquisition. KY and KH analyzed the data. All authors were involved in the interpretation of data, drafting of the manuscript, and provided critical feedback. All authors approved the final manuscript.
Funding This study was funded by AstraZeneca K.K.
Competing interests TE reports personal fees from AstraZeneca K.K., Chugai Pharmaceutical Co, Ltd, and MSD K.K. outside the submitted work. DA reports grants and personal fees from Taiho Pharmaceutical Co, Ltd and Chugai Pharmaceutical Co, Ltd, grants from ASKA Pharmaceutical Co, Ltd and Sanofi K.K., and personal fees from Nippon Kayaku Co, Ltd, Yakult Honsha Co, Ltd, Takeda Pharmaceutical Co, Ltd, Daiichi Sankyo Co, Ltd, MSD K.K., AstraZeneca K.K., Ono Pharmaceutical Co, Ltd, Kyowa Hakko Kirin Co, Ltd, and Janssen Pharmaceutical K.K. outside the submitted work. KH and MJ are employees of AstraZeneca K.K. HT reports grants and personal fees from Konica Minolta, and grants from Chugai Pharmaceutical Co, Ltd and Taiho Pharmaceutical Co, Ltd outside the submitted work.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data underlying the findings described in this manuscript may be obtained in accordance with AstraZeneca’s data sharing policy described at https://astrazenecagrouptrials.pharmacm.com/ST/Submission/Disclosure