Article Text

Abstract
Objectives In England, human papillomavirus (HPV) testing is to replace cytological screening by 2019–2020. We conducted a model-based economic evaluation to project the long-term clinical impact and cost-effectiveness of routine cytology versus HPV testing.
Methods An individual-based model of HPV acquisition, natural history, and cervical cancer screening was used to compare cytological screening and HPV testing with cytology triage for women aged 25–64 years (with either 3- or 5-year screening intervals for women aged under 50 years). The model was fitted to data from England's National Health Service Cervical Screening Programme. Both clinical and economic outcomes were projected to inform cost-effectiveness analyses.
Results HPV testing is likely to decrease annual cytology testing (by 2.76 million), cervical cancer incidence (by 290 cases), and health system costs (by £13 million). It may increase the number of colposcopies, although this could be reduced without leading to more cancers compared with primary cytology by increasing the interval between screens to 5 years. The impact in terms of quality-adjusted life-years (QALYs) depends on the quality of life weight given to colposcopies versus cancer.
Conclusions England's move from cytology to HPV screening may potentially be life-saving and cost-effective. Cost-effectiveness can be improved further by extending the interval between screens or using alternative triage methods such as partial or full genotyping.
- cervical cancer
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
HIGHLIGHTS
In England, human papillomavirus (HPV) testing is planned to replace cytological screening by 2019.
HPV testing is likely to decrease cervical cancer incidence and costs.
HPV testing may lead to more colposcopies and this may be mitigated with a longer screening interval.
Introduction
Persistent infection with a high-risk type of human papillomavirus (HPV) is a risk for cervical cancer. In England, as elsewhere, secondary prevention of cervical cancer has been based on cytological testing to detect cervical abnormalities since the introduction of the National Health Service Cervical Screening Programme (NHSCSP) in 1988. The incidence of new diagnoses of cervical cancer per 100 000 females (based on the 2013 European Standard Population) has fallen from 12.1 in 1995 to 9.4 in 2016. Currently, women aged 25–49 and 50–64 years receive invitations for screening every 3 and 5 years, respectively. Additionally, 12–13-year-old girls have been vaccinated against HPV since 2008, with coverage of the two-dose schedule above 80%.1
The development of rapid and sensitive tests for HPV now offers an alternative screening for cervical cancer. European trials of HPV testing as a primary cervical screening suggest that it provides 60%–70% greater protection against cervical cancer compared with cytology.2 Testing for high-risk HPV to determine management of women with borderline or low-grade abnormalities, and as a test-of-cure for recently treated women, has been used in England since 2011. In 2013, a pilot study of implementing screening in which the primary assessment is an HPV test was initiated at several sites across England. The National Screening Committee has agreed to replace cytological testing with HPV testing as the primary means of assessment England-wide by 2019, following a review of evidence including cost-effectiveness.3
HPV testing has higher sensitivity for high-grade lesion detection and provides stronger negative predictive power than cytology,4 leading to the possibility of extending the screening interval following a negative HPV test. Additionally, concern that primary HPV screening may lead to over-referral to colposcopy in young women, in whom there is a high prevalence of HPV infection, has led to discussions surrounding the introduction of additional triage tests prior to colposcopy.
To address these questions around the introduction of primary HPV testing in England, we conducted a model-based evaluation of the clinical impact and cost-effectiveness of switching from cytology to HPV testing for women aged 25–64 years, as well as increasing the standard screening interval from 3 to 5 years for women under 50 years of age. Our model has incorporated information on HPV acquisition, cervical disease progression, cancer incidence, and screening effectiveness.
Methods
A stochastic, individual-based simulation model (ie, a model which follows individual women in a population and has multiple random realizations) was developed to represent the natural history of cervical disease and potential impact of HPV- and cytology-based screening protocols. An overview of the model is shown in Figure 1; further technical details about the model structure and parameterisation are given in online supplementary Appendix A1-4. The model generates a cohort of women and simulates their lifetime history: (a) acquisition of HPV infection through partner acquisition and sexual transmission as a necessary pre-condition for cervical pathogenesis, (b) natural progression of HPV infection, cervical intra-epithelial neoplasia (CIN) and cervical cancer, and (c) screening attendance, detection, and treatment of cervical abnormalities through cervical screening according to the algorithms in online supplementary Appendix Figures A6-7. Eight high-risk HPV types (16, 18, 31, 33, 45, 51, 52, and 58) are separately modeled. Women can acquire multiple HPV infections, possibly simultaneously with different strains, and each infection follows its own timeline to clearance or emergence of a pre-invasive cancer lesion, adenocarcinoma, or squamous cell carcinoma. HPV vaccination was not incorporated, as most women currently eligible for screening in England are not vaccinated. Clinical outcomes (screening results, colposcopies, treatment of pre-cancerous lesions, invasive cancer, and death) over the lifetime of the women are tracked and used to calculate the cost-effectiveness of each screening strategy.
Supplemental material

Overview of model representation of human papillomavirus (HPV) transmission and progression to cancer for each of eight HPV types (16, 18, 31, 33, 45, 51, 52, and 58).
Three alternative screening strategies were considered for women aged 25–64 years: (a) cytological screening with HPV testing to determine further management of cytological abnormals ('primary cytology protocol'), with a 3-year (or 5-year for women over 50 years old) recall interval following a negative screen, which is the current screening practice in England; (b) HPV testing ('primary HPV protocol'), with cytological testing to determine further management of high-risk HPV positives, with a 3-year (or 5-year for women over 50 years old) recall interval following a negative primary screen; (c) HPV testing ('5-year primary HPV protocol') with an extended 5-year recall interval following a negative HPV screen, for all women regardless of age.
A cost-effectiveness analysis was conducted by comparing the incremental costs and quality-adjusted life-years (QALYs) over the lifetime of cohorts under different screening strategies. The reference case of the National Institute for Health and Care Excellence (NICE) was used.5 In particular, a healthcare provider perspective was used, costs were inflated to 2013/14 GBP (British Pound) using the Hospital and Community Health Services prices index, and discounting of 3.5% was used for both costs and QALYs. Probabilistic sensitivity analysis was conducted incorporating uncertainty in both epidemiologic and economic parameters.
The economic parameters used were estimated from the literature; they are summarized in Table 1, while their sources and derivation are explained in online supplementary appendix A5. Because quality of life weights for screening differed widely between studies, we conducted three separate analyses: (i) using weights from all preference-based utility studies identified,6–9 (ii) using weights from the study with the smallest screening-related detriments,7 and (iii) using weights from the study with the highest screening-related detriments.10 This work was conducted by Public Health England in order to inform decision-making by the NHSCSP.
Economic parameters used in the model
Results
HPV Testing
The model and best-fitting disease progression parameters are used to evaluate a change to the NHSCSP in England from primary cytology, the current protocol, to HPV testing, under the algorithm which is currently being implemented nationally.
Increased Number of Tests Performed Under HPV Testing
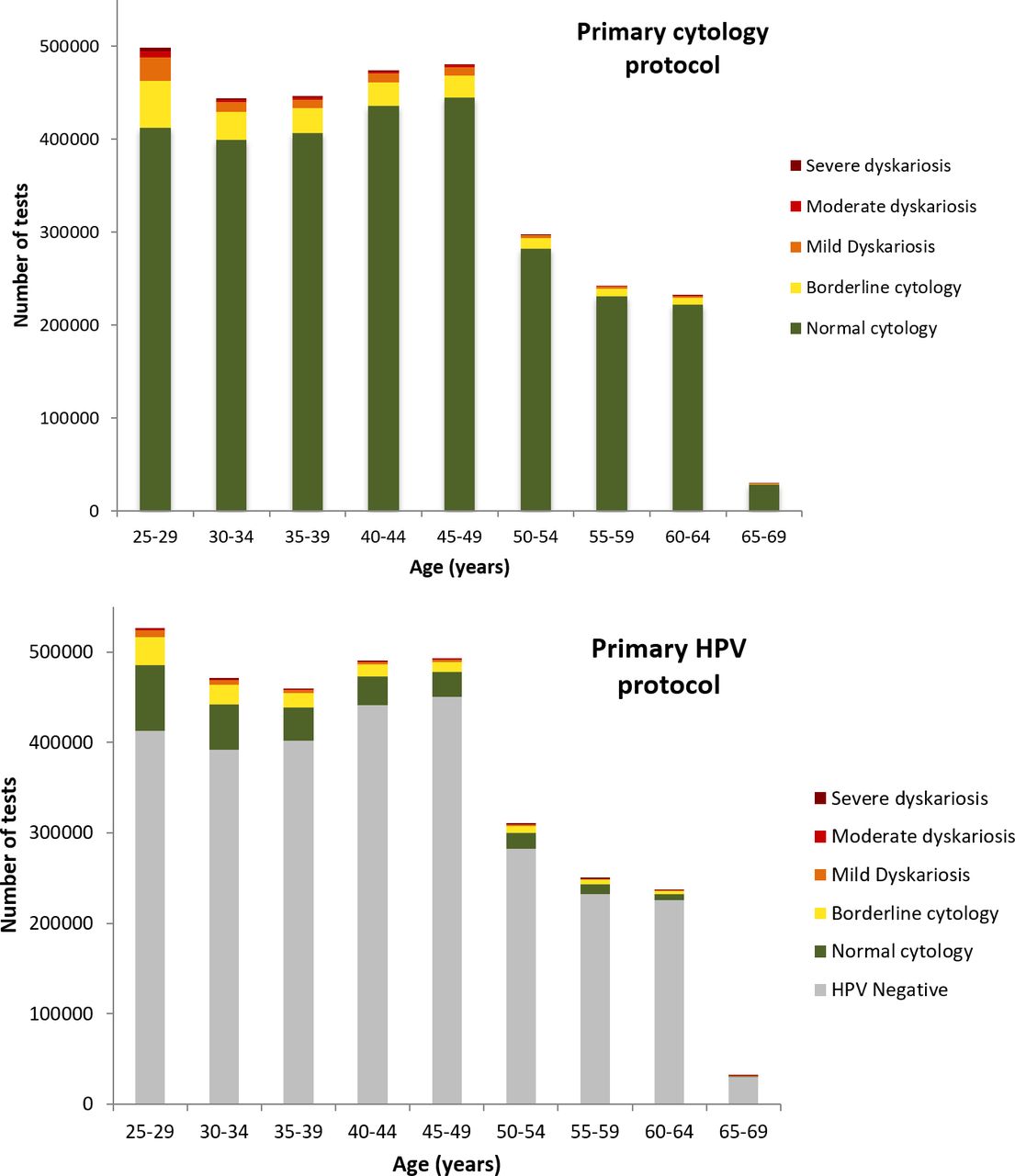
A summary of clinical outcomes under the HPV and cytology protocols is shown in Table 2 and figure 2. The annual number of primary screening tests is expected to increase by 5% under the standard HPV protocol from 3.14 to 3.31 million per annum; the largest increase is expected in women aged 25 to 35 years and represents an additional 73 000 tests on women that are followed after an HPV-positive result. A switch to the HPV protocol resulted in a reduction in the number of women undergoing cytological testing, from 3.14 to 0.38 million tests annually, while the proportion of women with positive cytology outcomes increased from 8.8% under cytology protocol to 35% under HPV protocol. A more detailed breakdown of number of tests and outcomes is shown for each screening strategy in the online supplementary Appendix.
Number of screening tests and colposcopies carried out each year (x10 000) under different screening protocols (mean and 95% CI), assuming 2013 population age distribution. Borderline indicates results that cannot definitely be classified as either normal or abnormal.
Number of women tested and predicted outcome under primary human papillomavirus (HPV) protocol and primary cytology protocol, assuming 2013 population age distribution in England.
Improved Efficiency of Screening Under HPV Testing
The model predicts a 25% increase in women referred to colposcopy through the screening program, as the HPV protocol has lower positive predictive value than the cytology protocol. The model does not consider women referred to colposcopy following a clinical indication. The number of grade 2 or worse CIN cases identified annually is expected to increase by 44%; reflecting 22 000 additional cases detected per year through the screening program. The referral value, that is the number of women referred to colposcopy, by way of the screening program, per detection of one CIN2 or worse lesion, is projected to decrease from 2.6 to 2.3. In addition to the increased ‘efficiency’ of colposcopy, the total number of primary screens required to identify a single case of CIN2 or worse lesions is also predicted to drop from 158 using cytology protocol, to 104 under HPV protocol.
Reduced Cancer Incidence and Cancer-related Deaths Under Primary HPV Testing
Best-fitting model simulations cover a wide range of scenarios for cancer incidence when we combine cases of squamous cell carcinoma and adenocarcinoma for HPV types 16,18, 31, 33, 51, 52, and 58 (Figure 3). The model predicts that a switch to HPV testing will result in a statistically significant decrease in the mean annual incidence of cervical cancer of 14.5%; equivalent to a reduction in 290 cases per year in individuals aged 10 to 79 years (95% CI 195 to 370). The number of cases detected in women aged 35+ years is expected to experience the largest drop, while the number of cases in women aged <30 years was not found to be significantly different between the two protocols. This corresponds to a mean reduction in cervical cancer-related deaths of 15.5%; 56 (range 38−75) fewer deaths are predicted under the HPV testing protocol. In terms of the ‘efficiency of primary screening’, we find that the HPV protocol requires an additional 587 screens per cancer case avoided.

{kind=link}
{kind=link}
{kind=link}
Cervical cancer incidence predicted by model under primary cytology and primary human papillomavirus (HPV) protocols. Boxes represent the interquartile prediction interval.
Cost Savings
A switch from cytology to the HPV protocol would lead to a total healthcare cost saving of £13 million (range £2.9−£22.8 million). The annual screening costs are expected to be £120.5 million. The discounted lifetime cost saving per women is estimated to be £14 (range £1−£27).
QALY Changes
We do not find substantial changes in QALYs gained associated with a switch from cytology to a HPV protocol. The median (95% CI) QALYs gained over the lifetime of a woman in the model was (i) −0.0026 (-0.0064 to 0.013) when using all utility studies, (ii) 0.0005 (−0.0013 to 0.0026)) when using the study with the smallest screening-related utility losses, and (iii) −0.0033 (−0.0004 to 0.0064) when using the study with the largest.
Extended Screening Interval
We consider the impact of increasing the recall interval, following a negative HPV screen, to 5 years for all women regardless of age (5-year primary HPV protocol). This fixed interval compares to current practice whereby women aged under 50 years are recalled at 3-year intervals, and women aged over 50 years are recalled at 5-year intervals. The model predicts that a switch from cytology to HPV testing with a 5-year interval for all women will lead to a 17% decrease in the number of primary tests carried out (Table 2). The model does not predict a significant difference in the number of colposcopies with a move from cytology to HPV with 5-year recall; however, the model predicts that more neoplasias will be detected per year. The increased ‘rate’ of detection per colposcopy under a 5-year protocol arises from the increased proportion of women attending colposcopy following a moderate or severe cytological referral. Overall, the increased detection and subsequent treatment of pre-cancerous lesions results in a decrease in cancer incidence by 145 (range 82−246) cases per year under the 5-year HPV protocol, saves 47 (range 27−67) lives per year, and saves 0.0008 discounted life-years per woman compared with cytology.
Moving from cytology to HPV testing, in combination with a regular 5-year screening interval, would lead to a substantial total healthcare cost saving of £33 million (range £23.7–£44.1 million). The annual screening costs are expected to be £97.7 million. The discounted lifetime cost saving per women is estimated to be £38 (range £25–£49).
Discussion
Our analysis suggests that a move from the current cytology to HPV screening without changing the recall interval will be both life-saving and cost-saving, with no significant difference in net QALYs gained. Such a move is expected to: (i) increase the number of screening tests performed, (ii) increase the number of colposcopy referrals, (iii) increase the number of lesions identified and treated through colposcopy, and (iv) decrease cervical cancer incidence and mortality.
Even if the shift to HPV screening is accompanied by an increase in the recall interval to 5 years, this is still expected to reduce cancer incidence, mortality, and costs. However, the reduction in cervical cancer mortality will be smaller. Despite the smaller reduction in deaths, the reduction in the number of colposcopies required means that a 5-year HPV protocol is more favorable in terms of net QALYs than a 3-year HPV protocol. Further reductions in colposcopies may be achievable by using alternative triage technologies (such as partial or full genotyping), although this was not modeled.
The cost-effectiveness of HPV testing in England was previously estimated using results from the ARTISTIC trial of HPV testing.11 This analysis also found HPV testing to be cost-effective and life-saving if accompanied by an increase in screening intervals to at least 5 years, but reached divergent outcomes in terms of the impact on QALYs depending on the assumptions made. Our analysis verifies and updates these results by using more recent screening and sexual behavior data, an independent model, and scenarios of direct interest to the National Screening Committee. A recent systematic review12 found that the majority of relevant model-based studies found HPV testing to be more cost-effective than cytology, which is in line with our results.
While the model reproduces HPV prevalence and cervical cancer incidence in the English population well, it does not capture a second peak in cancer incidence seen in women aged over 70 years. Cancers in older women are more likely to arise from high-risk HPV types rarely seen in cervical cancer, and not included in the model. Joste et al 13 showed that 100% of cancers in women aged under 30 years were attributable to modeled HPV types (16, 18, 31, 33, 45, 51, 52, and 58); however, this dropped to 75% in women aged over 40 years. Hence we may slightly underestimate the benefit of HPV testing in older women, since commercially available tests, such as the commonly used Hybrid Capture 2 assay, will also detect non-modeled types such as 35, 39, 56, 59, and 68. Another explanation for missing the second cancer peak is that it represents the effect of both cohort differences and age-related changes. The model calibration assumes that all women undergo screening according the current protocol from age 25 to 65 years. However, the NHSCSP began in 1988 so women aged 70+ years in the 2012 dataset would only have benefited from screening from age 45 years onwards. Model projections give a large uncertainty range around cancer incidence, representing the combined uncertainty from 16 distinct cancer-causing processes (eight HPV types leading to either squamous cell carcinomas or adenocarcinomas). Many of these HPV types are only rarely associated with cervical cancer in English women, so there are sparse data to constrain the underlying parameters.
We used costs from historical economic analyses of screening in England, inflated to 2014 values.11 The limitations of inflating historical costs are that we do not necessarily capture reduction in technology costs over time. Economies of scale also suggest that a switch to primary screening is likely to result in a reduction in the cost per HPV test. Overall, this will lead to further cost savings associated with a switch to HPV testing. Work on the detailed design and implementation of HPV testing is ongoing within the NHSCSP: this work includes developing appropriate education for professionals and information for patients.
There are large discrepancies in the literature for the utility detriments associated with cervical screening (particularly HPV-related screening) depending on the methodology used for eliciting utilities. We used sensitivity analyses to capture the extreme values reported in the literature; these suggest that the choice of utility values to use can determine whether an intervention is cost-effective in terms of its cost per QALY gained. This highlights the need for deeper understanding the QOL impact of screening, in order to appropriately judge what increase in colposcopies and pre-cancerous lesion treatments we are willing to accept in exchange for reductions in cervical cancer incidence and deaths.
The current analysis is based on a static model of infection, since changes in screening are unlikely to have a major effect on the rate at which women are infected with HPV. However, it is important to consider the implications of HPV vaccination (introduced in England in 2008) on HPV acquisition as vaccinated cohorts approach screening age. Further work needs to focus on identifying optimal screening strategies among both vaccinated and unvaccinated women among the age cohorts who were at the right age to be part of the national vaccination programme.
Ethics approval
Sexual behavior data were obtained from Natsal-3, which was granted ethical approval by the Oxfordshire Research Ethics Committee A (09/H0604/27). HPV prevalence data were collected from a study granted ethical approval by the South East Research Ethics Committee (07/H1102/97). Seroprevalence data were collected by the Health Protection Agency’s Seroepidemiology Unit, which holds ethical approval (05/Q0505/U5) to carry out serological surveillance in support of the National Immunization Programme for England and Wales, issued by the Joint University College London/University College London Hospitals (UCL/UCLH) Committees on the Ethics of Human Research. Cervical screening data were collected by Public Health England as part of public health surveillance conducted to monitor the HPV vaccination and cervical screening programs.
Acknowledgments
The authors thank Peter Sasieni, Alex Castenon, Rebecca Landy, Julietta Patnick, Henry Kitchener, Sue Moss, David Mesher, Koh Jun Ong, and the Bristol primary HPV pilot coordinators for many helpful discussions, feedback on previous iterations of this work, and sharing insight from their own data.
References
Footnotes
Contributors IB and MJ designed the study, carried out the analysis, interpreted the data, and drafted the manuscript with input from YC and KS. All authors contributed to manuscript review and approved the final version.
Funding This work was funded by Public Health England and the NHS Cervical Screening Programme (NHSCSP).
Competing interests KS works for the Blood Safety, Hepatitis, Sexually Transmitted Infections (STI) and HIV Service of Public Health England, which has provided GlaxoSmithKline plc with postmarketing surveillance reports on HPV infections which the companies are required to submit to the UK licensing authority in compliance with their Risk Management Strategy. A cost recovery charge is made for these reports.
Provenance and peer review Commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.