Article Text

Abstract
Objectives Optimal adjuvant treatment for early-stage clear cell and serous endometrial cancer remains unclear. We report outcomes for women with surgically staged International Federation of Gynecology and Obstetrics (FIGO) stage I clear cell, serous, and mixed endometrial cancers following adjuvant vaginal cuff brachytherapy with or without chemotherapy.
Methods From April 1998 to January 2020, women with FIGO stage IA–IB clear cell, serous, and mixed endometrial cancer underwent surgery and adjuvant vaginal cuff brachytherapy. Seventy-six patients received chemotherapy. High-dose rate vaginal cuff brachytherapy was planned to a total dose of 21 gray in three fractions using a multichannel vaginal cylinder. The primary objective was to determine the effectiveness of adjuvant vaginal cuff brachytherapy and to identify surgicopathological risk factors that could portend towards worse oncological outcomes.
Results A total of 182 patients were included in the analysis. Median follow-up was 5.3 years (2.3–12.2). Ten-year survival was 73.3%. Five-year cumulative incidence (CI) of vaginal, pelvic, and para-aortic relapse was 1.4%, 2.1%, and 0.9%, respectively. Five-year locoregional failure, any recurrence, peritoneal relapse, and other distant recurrence was 4.4%, 11.6%, 5.3%, and 6.7%, respectively. On univariate analysis, locoregional failure was worse for larger tumors (per 1 cm) (HR 1.9, 95% CI 1.2 to 3.0, p≤0.01). Any recurrence was worse for tumors of at least 3.5 cm (HR 3.8, 95% CI 1.3 to 11.7, p=0.02) and patients with positive/suspicious cytology (HR 4.4, 95% CI 1.5 to 12.4, p≤0.01). Ten-year survival for tumors of at least 3.5 cm was 56.9% versus 86.6% for those with smaller tumors (HR 2.9, 95% CI 1.4 to 5.8, p≤0.01). Ten-year survival for positive/suspicious cytology was 50.9% versus 77.4% (HR 2.2, 95% CI 0.9 to 5.4, p=0.09). Multivariate modeling demonstrated worse locoregional failure, any recurrence, and survival with larger tumors, as well as any recurrence with positive/suspicious cytology. Subgroup analysis demonstrated improved outcomes with the use of adjuvant chemotherapy in patients with large tumors or positive/suspicious cytology.
Conclusion Adjuvant vaginal cuff brachytherapy alone without chemotherapy is an appropriate treatment for women with negative peritoneal cytology and small, early-stage clear cell, serous, and mixed endometrial cancer. Larger tumors or positive/suspicious cytology are at increased risk for relapse and worse survival, and should be considered for additional upfront adjuvant treatments, such as platinum-based chemotherapy.
- endometrial neoplasms
- radiation oncology
Data availability statement
Data are available upon reasonable request. Research data are stored in an institutional repository and will be shared upon request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
HIGHLIGHTS
Tumor size and peritoneal cytology should be obtained in early-stage, high-risk histology endometrial cancer.
Adjuvant vaginal cuff brachytherapy alone provides long-term oncological control in women with small tumors and negative peritoneal cytology.
Positive peritoneal cytology and larger tumors are at higher risk and should be considered for upfront additional adjuvant therapies, such as cytotoxic chemotherapy.
Introduction
Endometrial cancer remains the most common gynecological malignancy in the United States.1 Serous and clear cell histologies represent a rarer hormone-independent, aggressive subtype,2 which have been associated with higher rates of extra-uterine spread, as well as higher rates of recurrence.3 4 Treatment recommendations for early-stage endometrioid uterine cancer (International Federation of Gynecology and Obstetrics (FIGO) stage I) have been established through historical randomized clinical trials.5–8 However, the optimal treatment for serous and clear cell histologies remains unclear. These patients were excluded from enrollment on pivotal early-stage trials,5 7 8 and when included, represented less than 1% of patients enrolled.6
More recent clinical trials have included these rarer histologies. The GOG-249 trial, which randomized patients with high-risk FIGO stage I and II endometrial cancers after total abdominal hysterectomy, bilateral salpingo-oopherectomy, and either lymph node dissection or postoperative imaging for lymph node assessment to pelvic radiotherapy versus vaginal cuff brachytherapy coupled with chemotherapy.9 Serous and clear cell cancers combined constituted 19.3% of the study cohort. The PORTEC-3 trial randomized women with FIGO stage I–III high-risk endometrial cancers to adjuvant chemoradiotherapy versus adjuvant pelvic radiotherapy alone.10 Clear cell and serous cancers represented approximately 16% and 10% of the overall population, respectively.10 In PORTEC-3, early-stage disease only represented just over a quarter of the serous population.10 However, in both these trials, further detailed clinical and pathological characteristics are not available for the subset of patients with serous and clear cell cancers. Thus, despite inclusion in recent randomized trials, the minutiae of details of which high-risk population patients were included are not readily available for assessment, leaving ambiguity in discerning appropriate adjuvant therapies in specifically early-stage high-risk histologies. A recent SEER analysis of patients with FIGO I–II serous (n=947) and clear cell (n=241) cancers noted no clear trend in adjuvant therapy recommendations.11 Brachytherapy, chemotherapy, and external beam were utilized in 36%, 51%, and 31% of patients, respectively.11
Since 1998, our institutional practice has been to treat women with surgically staged FIGO stage I serous or clear cell cancers after total abdominal hysterectomy, bilateral salpingo-oopherectomy, pelvic and para-aortic lymph node evaluation, omentectomy, peritoneal washings for cytology, and random peritoneal biopsies with vaginal cuff brachytherapy alone with or without chemotherapy. Our approach has previously been published and demonstrated favorable outcomes, alongside similar retrospective series12–14; however, all were lacking meaningful univariable and multivariable modeling. Here, we present long-term outcomes using this treatment approach to aid in developing appropriate adjuvant therapy recommendations for this specialized cohort
Methods
Patients
This retrospective study was performed under institutional review board approval utilizing an institutional database of patients treated with postoperative vaginal cuff brachytherapy for a diagnosis of FIGO stage IA or IB serous or clear cell cancer. The requirement for written informed consent was waived by the Istitutional Review Board. From April 1998 to January 2020, 182 women were identified as having received adjuvant high-dose rate vaginal cuff brachytherapy without external beam radiotherapy following surgical intervention. All patient characteristics and treatment-related details were verified through review of the electronic medical record. Patients included in our prior publication12 were re-reviewed with updated follow-up. All patients were staged according to 2009 FIGO staging guidelines.15 Three distinct histologies were included: serous, clear cell, and mixed (both serous and clear cell). Tumor histologies that demonstrated endometrioid with serous or clear cell were included if more than 10% of the tumor demonstrated aggressive histological variant and were classified based on the aggressive component.
Treatment
Patients underwent total abdominal hysterectomy, bilateral salpingo-oopherectomy with pelvic and para-aortic lymph node dissection (prior to 2014), or bilateral sentinel lymph node biopsy (after 2014), omentectomy, pelvic cytology, and peritoneal biopsies. Prior to 2007, patients underwent open surgery, with a transition for most patients to laparoscopic or robotic assisted procedures thereafter.
Adjuvant vaginal cuff brachytherapy was delivered after appropriate healing was determined by physical exam. A high-dose rate technique was used in a dedicated outpatient radiation oncology brachytherapy suite. High-dose rate vaginal cuff brachytherapy was planned to a total dose of 21 gray in three fractions using a multichannel vaginal cylinder.16 A CT scan was obtained prior to the first fraction to assess for appropriate placement and for computation of dose to surrounding organs at risk. The prescription dose was prescribed 5 mm distal to the tip of the applicator, 5 mm anterior and posterior, and 7 mm lateral to the applicator.16 The prescription dose was tapered to the surface of the applicator at 1 cm proximal to the end of the vaginal canal. Patients were treated on non-consecutive weekdays over 5–8 days.
Patients were discussed in a multi-disciplinary fashion and referred to medical oncology when deemed appropriate by the team, weighing pathological extent of disease with patient comorbidities. Routine follow-up typically consisted of pelvic exam every 3 months and imaging (usually CT abdomen and pelvis) every 6 months for up to 2 years. After 2 years, patients were followed with pelvic exam alone every 6–12 months.
Outcomes
The primary objective of this study was to determine the effectiveness of adjuvant vaginal cuff brachytherapy and to identify surgicopathological risk factors that could portend towards worse oncological outcomes. Endpoints collected included vaginal recurrence, pelvic recurrence, para-aortic recurrence, distant recurrence, and survival. Median (interquartile range (IQR)) time to event was calculated for patient and treatment-related variables. When comparing subgroups of patients, the Wilcoxon rank sum test and χ2 test were used to compare baseline patient and treatment-related variables.
All outcomes were measured from the date of the vaginal cuff brachytherapy fraction. Overall survival was estimated using the Kaplan-Meier method. Competing risk models were used to report cumulative incidences (CIs) of vaginal recurrence, pelvic recurrence, para-aortic recurrence, locoregional failure, and distant relapse. Locoregional failure was defined as vaginal, pelvic, or para-aortic nodal failure. Univariate associations between patient, treatment, and pathological factors with overall survival, locoregional failure, or any failure were identified using the Cox proportional hazards model. The calculated median was utilized for dichotomizing data in analyses for age, time from surgery to implant, and tumor size. Tumor size was additionally run as a continuous variable for analysis. To minimize statistical error, given the overall low event rate, only associates that were significant or near significance in univariate modeling were analyzed in a multivariate model.
An ad hoc test for interaction was done to determine any interaction between chemotherapy receipt and significant variables (between the chemotherapy and non-chemotherapy patient cohorts) as it pertains to patient outcomes. A subgroup analysis regarding the impact of chemotherapy on oncological outcomes (through Kaplan-Meier and competing risk models) was completed on high-risk cohorts, identified as statistically significant variables from univariate and multivariate modeling. A generated p-value of up to 0.05 was chosen for statistical significance. Data were analyzed using SAS version 9.4. In accordance with the journal’s guidelines, we will provide our data for the reproducibility of this study in other centers if requested.
Results
Patient and Treatment Characteristics
Baseline patient and treatment characteristics are summarized in Table 1. Median follow-up time was 5.3 years (2.3–12.0). Patients treated after 2014 received sentinel lymph node evaluation, representative of an institutional transition in surgical management. Few patients (n=9, 4.9%) had no lymph node evaluation. Reasons for no pelvic lymph node dissection included morbid obesity (n=2), intraoperative emergency (n=1), incidental oncological diagnosis with patient declining surgical staging (n=2), surgeon discretion (n=3), and unknown due to outside surgery (n=1).
Patient and treatment characteristics
Seventy-four patients (40.7%) received random biopsies of other suspicious areas during surgery, all of which were negative for disease. Nearly all patients had omental exploration (77.5%) and peritoneal cytology (87.9%). Pathological characteristics are given in Table 2. Pathological tumor size was available for 92% of patients. Median size of the tumor in the hysterectomy specimen was 3.4 cm. Eighteen per cent had lymphovascular space invasion, while 14.3% of patients had positive (12.6%) or suspicious (1.7%) peritoneal cytology.
Pathological characteristics
All but one patient received 21 gray in three fractions every other day. One patient received 14 gray in two fractions without any known indication of toxicity before withdrawing consent for treatment. Vaginal brachytherapy was delivered a median time of 6.4 weeks after surgery (5.0–7.7 weeks). Seventy-six patients received chemotherapy (41.8%), most commonly after brachytherapy completion (n=69, 90.8%), and consisting of four to six cycles of carboplatin and paclitaxel. Baseline demographics of patients receiving chemotherapy versus those who did not are given in the Online supplemental material. In brief, patients receiving chemotherapy were more likely to have FIGO stage IB disease, have larger tumors, and have positive or suspicious cytology.
Supplemental material
Locoregional Disease Recurrence
Three patients (1.6%) experienced vaginal recurrence. The cumulative incidence (95% CI) of vaginal relapse at 5 and 10 years was 1.4% (0.3% to 5.4%) and 2.5% (0.8% to 8.0%), respectively. Two patients had recurrent disease in the vagina alone and one had synchronous lung metastases. Both patients with isolated vaginal recurrences were treated successfully and are alive at the time of last follow-up. Three patients (1.6%) had recurrence elsewhere in the true pelvis (two at the pelvic sidewall and one in a pelvic lymph node). One patient had recurrent disease in a para-aortic lymph node (0.5%). Of these four patients, three had synchronous distant recurrence (two in the peritoneum and one in the lungs). The 5-year cumulative incidence of pelvic relapse and para-aortic relapse was 2.1% (0.7% to 6.7%) and 0.9% (0.1% to 6.4%), respectively. The cumulative incidence of locoregional failure at 5 and 10 years is 4.4% (2.0% to 9.8%) and 5.5% (2.6% to 11.7%), respectively.
Extrapelvic Disease Recurrence
Fourteen patients had distant recurrence, including seven patients within the peritoneum. Ten of the 14 women had recurrence with distant failure alone. The 5- year cumulative incidence of peritoneal and non-peritoneal metastasis was 5.3% (2.5% to 11.2%) and 6.7% (3.5% to 12.8%), respectively. There were no trends in histology subtype for peritoneal or other distant metastases. At last follow-up, 50% of these 14 patients had died from recurrent uterine disease, with the exception of one patient who died from diffuse metastatic breast cancer.
Any Recurrence andSurvival
The cumulative incidence of any recurrence at 5 and 10 years was 11.6% (7.2% to 18.6%) and 12.7% (8.0% to 20.1%), respectively. The overall survival at 10 years for all patients was 73.3% (64.6% to 82.9%).
Univariate COX Modeling
An ad hoc analysis of interaction between chemotherapy and FIGO stage, chemotherapy and size, and chemotherapy and cytology as it pertains to locoregional recurrence, extrapelvic recurrence, any recurrence, and overall survival demonstrated no statistically significant interactions. Therefore, modeling of variables for risk was analyzed within all patients. Table 3A demonstrates variables of statistical and non-statistical significance on univariate Cox modeling.
Univariate associates
Locoregional failure was seen with larger tumors (size per centimeter) (Table 3A). Of the six patients with locoregional failure, all patients had tumors of at least 3.5 cm. The cumulative incidence of locoregional failure at 5 years for those with tumors of at least 3.5 cm versus those with tumors less than 3.5 cm was 7.9% (3.4% to 18.6%) versus 1.3% (0.2% to 9.2%), respectively (Figure 1B; Table 3A). No additional clinical factors, including positive peritoneal cytology, were associated with increased locoregional failure. The cumulative incidence of locoregional failure at 5 years for those with positive/suspicious versus negative cytology was 4.9% (0.7% to 33.1%) versus 4.0% (1.5% to 10.7%), respectively (Figure 1A; Table 3A).
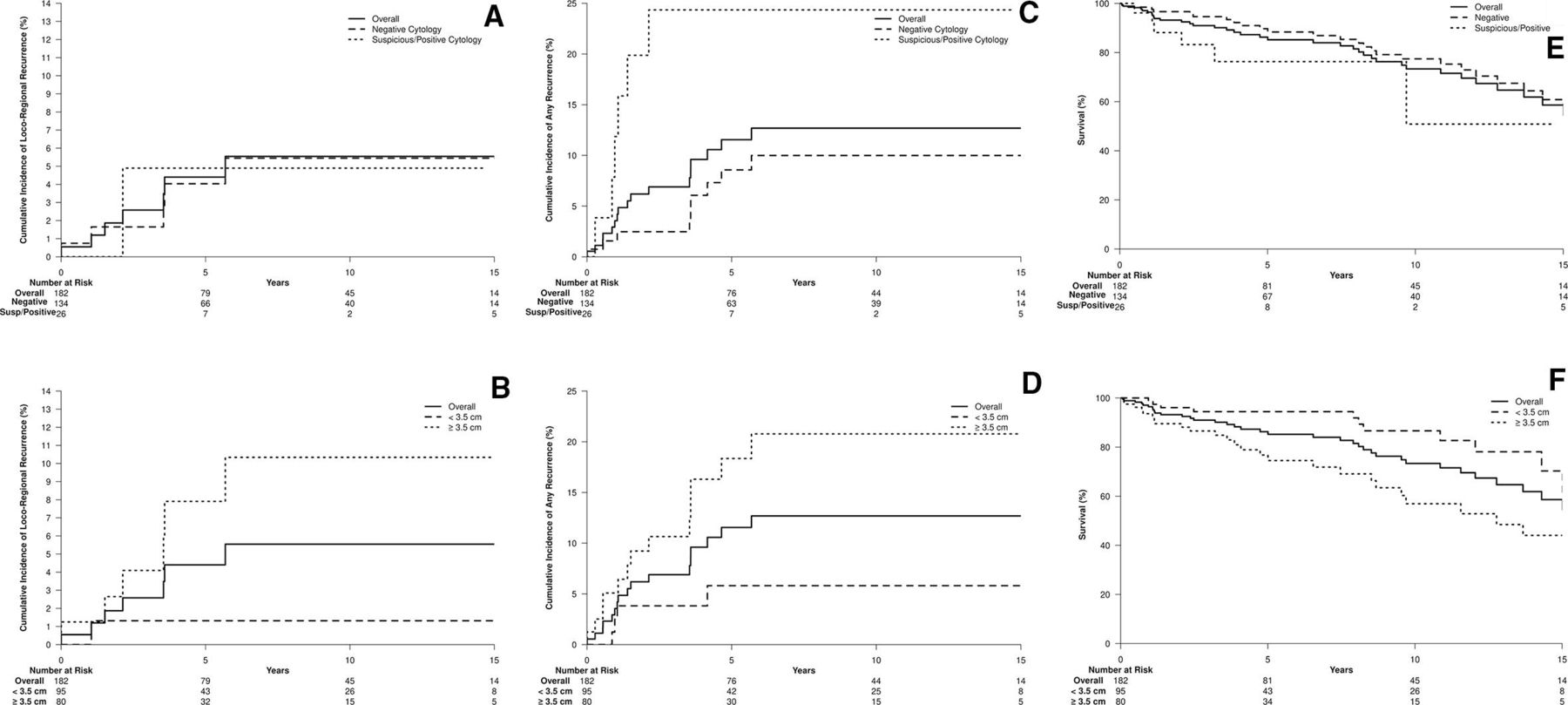
Locoregional recurrence (all patients) categorized by high-risk features: (A) cytology, (B) size. Any recurrence (all patients) categorized by high-risk features: (C) cytology, (D) size. Overall survival (all patients) categorized by high-risk features: (E) cytology, (F) size.
A significant risk of any failure was seen with older women, larger tumors (≥3.5 cm and size as a continuous variable), and positive/suspicious cytology. The cumulative incidence of any recurrence at 5 years for those with tumors of at least 3.5 cm versus those with tumors less than 3.5 cm was 18.4% (10.9% to 31.0%) versus 5.8% (2.2% to 15.4%), respectively (Figure 1D; Table 3A). The cumulative incidence of any recurrence at 5 years for those with positive/suspicious versus negative cytology was 24.4% (12.1% to 49.0%) versus 8.6% (4.4% to 16.9%), respectively (Figure 1C; Table 3A). For the entire cohort of 182 patients, chemotherapy was not associated with an improvement in locoregional or any failure.
No survival benefit was seen with adjuvant chemotherapy, but survival was statistically worse for older patients with larger tumors (≥3.5 cm and size as a continuous variable), with a trend towards worse overall survival in those with positive/suspicious cytology (p=0.09) (Table 3A). Overall survival at 10 years for those with tumors of at least 3.5 cm versus those with tumors less than 3.5 cm was 56.9% (43.0% to 74.2%) versus 86.6% (76.5% to 97.0%), respectively (Figure 1F; Table 3A). Overall survival at 10 years for those with positive/suspicious versus negative cytology was 50.9% (22.0% to 100.0%) versus 77.4% (67.9% to 87.6%), respectively (Figure 1E; Table 3A).
Multivariate COX Modeling
Multivariate modeling demonstrated a statistical improvement in locoregional failure with smaller tumors (size as a continuous variable) (Table 3B). Improvement in any failure was seen with negative cytology and smaller tumors (size as a continuous variable) (Table 3B) and overall survival was worse for patients with larger tumors (≥3.5 cm and size as a continuous variable) and positive/suspicious cytology (Table 3B).
Multivariate models (top: utilizing size as a continuous variable; and bottom: utilizing dichotomized data by median size)
Subgroup Analysis
Patients with positive/suspicious peritoneal cytology (n=26) had similar median age at diagnosis and size of tumor compared with the overall cohort. These patients underwent similar surgical and radiotherapy interventions. Of the 26 patients, 20 patients received chemotherapy and six patients did not. Of the 20 patients who received chemotherapy, only one patient (5.0%) experienced failure and died of disease. This is compared with five of six patients (83.3%) who did not receive chemotherapy and subsequently had recurrent disease. At last follow-up, two of these five patients had died from disease (Online supplemental material).
The 5- year cumulative incidence of locoregional failure for patients with positive/suspicious cytology who received chemotherapy versus no chemotherapy was 0% versus 27.8% (5.4% to 100%), respectively (Figure 2A; HR 0.04, 95% CI <0.001 to 4.13). The 5-year cumulative incidence of any recurrence for patients with positive/suspicious cytology who received chemotherapy versus no chemotherapy was 5.3% (0.8% to 35.5%) versus 83.3% (58.3% to 100%), respectively (Figure 2C; HR 0.04, 95% CI 0.005 to 0.36). The 5- year overall survival for patients with positive/suspicious cytology who received chemotherapy versus no chemotherapy was 80.5% (59.2% to 100%) versus 55.6% (23.1% to 100%), respectively (Figure 2E; HR 0.37, 95% CI 0.06 to 2.22).

{kind=link}
{kind=link}
Locoregional regional recurrence for high-risk cohorts ((A) cytology, (B) size) with and without the receipt of chemotherapy. Any recurrence for high-risk cohorts ((C) cytology (D) size) with and without the receipt of chemotherapy. Overall survival for high-risk cohorts ((E) cytology, (F) size) with and without the receipt of chemotherapy. P value represents the difference in outcome between the receipt or omission of chemotherapy.
A secondary analysis of the patients with tumors of at least 3.5 cm demonstrated a similar trend. Eighty patients with a median age of 68 years had tumors above this dichotomized size variable. Seventeen (21%) patients were noted to have positive/suspicious peritoneal cytology. Forty-two of these patients received chemotherapy (51.9%), 3 of whom developed recurrences (all distant), for a 7% rate of failure in those with large tumors who received chemotherapy. None of these patients with recurrences also had positive/suspicious cytology. This is compared with the 48.1% (n=38) of patients with tumors of at least 3.5 cm who did not receive chemotherapy. Among these chemo-naïve patients (n=38), there were 11 failures (28.2%). Eight of 11 patients had distant recurrence, five with synchronous locoregional recurrence. The other three had recurrence with locoregional disease alone.
The 5-year cumulative incidence of locoregional failure for patients with tumors of at least 3.5 cm who received chemotherapy versus no chemotherapy was 0% versus 15.3% (6.8% to 34.5%), respectively (Figure 2B; HR 0.07, 95% CI 0.003 to 1.66). The 5-year cumulative incidence of any recurrence for patients with tumors of at least 3.5 cm who received chemotherapy versus no chemotherapy was 7.3% (1.8% to 29.8%) versus 29.6% (17.5% to 50%), respectively (Figure 2D; HR 0.17, 95% CI 0.04 to 0.76). The 5-year overall survival for patients with tumors of at least 3.5 cm who received chemotherapy versus no chemotherapy was 81.8% (68.2% to 96.%7) versus 72.0% (57.4% to 89.7%), respectively (Figure 2F; HR 0.61, 95% CI 0.27 to 1.38).
A group defined as the lowest risk group, based on univariate modeling, includes patients with tumors less than 3.5 cm and negative cytology (n=65). Of these patients, 22 received chemotherapy and 43 patients did not. There were two failures in the non-chemotherapy arm and 0 failures in the chemotherapy arm. On analysis, there was no trend or statistically significant difference in locoregional failure (p=0.92), any recurrence (p=0.77), or overall survival (p=0.48) in this cohort of patients who received or did not receive adjuvant chemotherapy.
Discussion
Summary of Main Results
For 22 years, our institutional approach has been to treat patients with surgically staged FIGO stage I clear cell or serous cancers with vaginal cuff brachytherapy alone with or without chemotherapy. Given the longevity of this patient population, longer term follow-up is warranted to demonstrate clear oncological outcomes and patterns. At a median follow-up of 5.3 years, 5-year and 10-year rates of locoregional failure are small at 4.4% and 5.5% and any recurrence at 11.6% and 12.7%. Long-term follow-up demonstrates a 10-year overall survival of 73.3%. In our analyses, disease outcomes were negatively impacted for all analyzed histologies in the setting of positive/suspicious peritoneal cytology or larger tumors (per 1 cm and ≥3.5 cm), irrespective of invasiveness or polyp-confined disease. We conclude that vaginal cuff brachytherapy is a reasonable option in appropriately selected women with surgically staged, high-risk, early-stage endometrial cancer; however, this analysis demonstrates a clear trend in pathological factors that portend to worse disease control and long-term survival, which should be considered for escalation of care. Our data suggest that the role of chemotherapy in the entire patient population is without benefit, but should be considered to improve outcomes in the setting of these aforementioned negative pathological factors.
Results in the Context of Published Literature
Two historical randomized trials demonstrated improvement in locoregional control without an improvement in overall survival with the use of adjuvant radiotherapy after surgical intervention for early-stage type I uterine-confined cancer.5 6 Two-thirds of recurrences were located in the vaginal cuff and thus a subsequent trial established vaginal cuff brachytherapy as the standard of care for women with high to intermediate risk FIGO stage I endometrioid endometrial cancer.7 8
While these trials paved the way for adjuvant therapy in early-stage endometrioid cancer, high-risk histologies were not represented or highly underrepresented in these studies. However, in GOG-249,9 high-risk histologies, in the setting of negative peritoneal cytology, were adequately represented in the two arms with failure rates as follows: serous 15.3% (pelvic radiotherapy) versus 14.0% (vaginal cuff brachytherapy/chemotherapy) and clear cell 5.0% (pelvic radiotherapy) and 4.3% (vaginal cuff brachytherapy/chemotherapy). Similar to randomized trials in early-stage endometrial cancer,7 8 the cumulative incidence of recurrence in the pelvic and para-aortic nodes in GOG-249 was higher with vaginal cuff brachytherapy/chemotherapy compared with pelvic radiotherapy (9% vs 4%, HR 0.47, 95% CI 0.24 to 0.94) without a difference in vaginal or distant recurrence. The risk of pelvic and para-aortic recurrence was distributed evenly across histologies. Most pertinent from this study is that patients with serous histology represented 29% of recurrences, while only representing a small proportion of the histology, suggesting that additional nuanced pathological risk factors need to be considered for these histologies to determine who benefits from which adjuvant therapy.9
Additionally, the three largest surgically staged retrospective studies specific to early-stage, high-risk histology endometrial cancer were published in 2012–201312–14 and demonstrated a lack of clarity in surgicopathological prognostic factors on variable modeling for type II endometrial cancer.
Our data demonstrate an important factor is pathological tumor size. While the trend in worse oncological outcomes with increasing size of tumor is well established across many disease sites, it is pertinent to note its clinical relevance in uterine-confined malignancies as size of tumor is not routinely reported. Recent recommendations published in the International Journal of Gynecologic Pathology regarding the processing of endometrial carcinomas17 highlights the lack of clarity regarding the importance of reporting the size of the tumor. Some studies have suggested the importance of tumor size on lymph node metastases and oncological outcomes,18–22 while others demonstrated no clear significance compared with alternative risk factors, such as depth of invasion.23 24 Importantly, these studies focused on mainly type I histologies, and no study has provided data regarding the importance of specimen size specifically in a high-risk histology cohort.
An additional piece of prognostic information demonstrated in our data is peritoneal cytology, yet the role of obtaining peritoneal cytology has been questioned. Prior to the 2009 FIGO staging, positive peritoneal cytology was a defining staging variable, upstaging women with stage I or stage II endometrial to stage IIIA disease even in the presence of no extrauterine extension.15 While some studies have suggested prognostic implications with positive cytology,25 others have refuted the association of positive cytology with worse oncological outcomes.26 Additional studies have further obfuscated the prognostic significance of positive peritoneal cytology, citing it as both a dependent risk factor (attributable to other adverse features) or an independent variable.27 28 Similar to the studies available on size of tumor, the role of cytology in high-risk histologies has not been individually investigated. Given the lack of clarity, the revised 2009 FIGO staging criteria removed positive cytology from the staging matrix15 and at many centers peritoneal cytology is likely no longer obtained.
Implications for Practice and Future Research
In this analysis of a large cohort of patients with long-term follow-up, we demonstrate the prognostic significance of tumor size and peritoneal cytology, and therefore recommend obtaining peritoneal cytology at the time of surgical intervention, and reporting the size of tumor in the surgical pathology report to guide appropriate selection of adjuvant therapies.
These results suggest that the presence of suspicious/positive cytology or larger tumor size warrant treatment escalation. Our data suggest the use of platinum-based chemotherapy may be appropriate escalated therapy in these patients because the use of chemotherapy in these subgroups demonstrated improved disease control and a trend toward improved overall survival. In the setting of negative cytology and small endometrial-confined tumors, these data support the use of vaginal brachytherapy alone as the role of chemotherapy in this cohort did not directly impact any oncological outcome.
While this study demonstrates the efficacy of vaginal cuff brachytherapy in appropriately selected stage I high-risk endometrial cancer, further research is warranted. While there was a single patient with pelvic failure alone, a comparison study with patients receiving pelvic external beam radiotherapy alone could provide valuable data, including oncological outcomes, patient-reported outcomes, and quality of life metrics to help guide optimal adjuvant therapy. Additionally, optimal systemic therapy and optimal number cycles of chemotherapy cannot be discerned from these data, but warrant further investigation to balance outcomes against toxicity. Consideration of molecular profiling in this cohort is also warranted to further optimize and individualize care. Currently, the role of targeted therapeutic agents, in early and late stage uterine serous cancers that express human epidermal growth factor 2 (HER2), is being studied, with favorable outcomes.29 30 However, despite the move into molecular profiling, at this time, this is not readily available at all treatment centers. PORTEC-431 is currently accruing and will randomize women with early-stage endometrial cancer to adjuvant therapy based on integrated molecular risk profile versus vaginal brachytherapy alone; however, women with high-risk histologies will not be enrolled in this study.
Strengths and Weaknesses
This study of a large cohort of patients with significant follow-up demonstrates clear oncological trends; however, it does have several limitations. Predominantly, it is a retrospective study in patients treated over a 22-year timeframe. There is a lack of racial diversity in the patient population. The 22-year timeframe implicates heterogeneity in surgical and referral patterns. Additionally, even with significant follow-up, the event rate remains low. The majority of the patients were FIGO stage IA and while no discernible difference in outcomes was seen on univariate analysis in patients with no residual disease (n=10), polyp-confined disease (n=22), no invasive disease (n=54), or at least 50% invasive disease (FIGO stage IB; n=22), the overall event rate was low, and therefore, these cohorts warrant further investigation. Additionally, while no difference in outcomes was seen between histologies, including patients with both serous and clear cell cancers added to the heterogeneity of the patient population. Five per cent of patients did not receive lymph node evaluation, which is similar to the rate in GOG-249.9 There was no additional risk seen in these patients because only one patient had recurrence, in the peritoneum, and had positive cytology and a 4.7 cm tumor, and did not receive chemotherapy. Notably, a low event rate leads to the inability to conduct robustly powered subgroup and multivariate analyses. In univariate and multivariate analyses, size was deemed prognostic as a continuous variable, but when dichotomized from the median (≥3.5 cm), not all analyzed outcomes remained significant. This raises the question of whether 3.5 cm is the appropriate size cut-off to warrant concern. Notably, this cohort would benefit from randomized clinical evidence in order to discern appropriate management for these patients; however, given the rarity of these histologies and the low event rate in this disease, a clinical trial would be difficult to execute in a reasonable time frame.
Conclusions
Women with early-stage serous and clear cell endometrial cancer should be considered for vaginal brachytherapy alone after appropriate surgical intervention with a thorough pathological analysis. This analysis should include tumor size assessment, lymph node evaluation, and peritoneal cytology analysis. Patients with positive peritoneal cytology or large tumors, suggestive of tumor size greater than 3.5 cm, should be considered a higher risk cohort and be considered for vaginal cuff brachytherapy and further escalation of care, such as adjuvant chemotherapy.
Data availability statement
Data are available upon reasonable request. Research data are stored in an institutional repository and will be shared upon request to the corresponding author.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ejeansMD
Contributors All aforementioned authors contributed to the design and implementation of the research, to the analysis of the results and to the writing of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.