Article Text

Abstract
Objective Despite good prognosis for patients with low-risk endometrial cancer, a small subset of women with low-grade/low-stage endometrial cancer experience disease recurrence and death. The aim of this study was to characterize clinical features and mutational profiles of recurrent, low-grade, non-myoinvasive, ‘ultra-low risk’ endometrioid endometrial adenocarcinomas.
Methods We retrospectively identified patients with International Federation of Gynecology and Obstetrics (FIGO) stage IA endometrioid endometrial cancers who underwent primary surgery at our institution, between January 2009 and February 2017, with follow-up of ≥12 months. ‘Ultra-low risk’ was defined as FIGO tumor grade 1, non-myoinvasive, and lacking lymphovascular space invasion. Tumor-normal profiling using massively parallel sequencing targeting 468 genes was performed. Microsatellite instability was assessed using MSIsensor. DNA mismatch repair (MMR) protein proficiency was determined by immunohistochemistry.
Results A total of 486 patients with ultra-low risk endometrioid endometrial cancers were identified: 14 (2.9%) of 486 patients developed a recurrence. Median follow-up for non-recurrent endometrioid endometrial cancers: 34 (range 12–116) months; for recurrent endometrioid endometrial cancers: 50.5 (range 20–116) months. Patients with recurrent disease were older, had lower body mass index, and were most commonly non-White (p=0.025, p<0.001, and p<0.001, respectively). Other clinical characteristics did not differ. MMR immunohistochemistry was obtained for 211 (43%) tumors: 158 (75%) MMR-proficient and 53 (25%) MMR-deficient. Primary tumors of 9 recurrent and 27 non-recurrent endometrioid endometrial cancers underwent mutational profiling. Most were microsatellite stable (6/9, 67% recurrent; 25/27, 93% non-recurrent). Recurrent PTEN and PIK3CA mutations were present in both groups. Exon 3 CTNNB1 hotspot mutations were found in 4/9 (44%) recurrent and 8/27 (30%) non-recurrent (p=0.44).
Conclusions Patients diagnosed with ultra-low risk endometrioid endometrial cancers have an overall excellent prognosis. However, in our study, 2.9% of patients with no identifiable clinical or pathologic risk factors developed recurrence. Further work is warranted to elucidate the mechanism for recurrence in this population.
- endometrial neoplasms
- genital neoplasms, female
Statistics from Altmetric.com
Highlights
Ultra-low risk endometrioid endometrial cancer recurrence rate is 2.9%.
No identifiable clinical or pathologic risk factors were noted.
Tumor genomic profile did not reveal differences between recurrent and non-recurrent tumors.
Introduction
Endometrial cancer is the most common gynecologic malignancy in the United States, diagnosed in over 60 000 women annually1 The majority of these women are diagnosed with low-grade, uterine-confined disease and have an excellent 5-year survival of over 90%.1 However, despite this generally good prognosis, a small subset of women with low-grade/low-stage endometrial cancer experience disease recurrence and death. The recurrence rate for early-stage disease across histologic subtypes varies widely, from 2% to 26% in the reported literature.2
Previous studies have examined risk factors for recurrence among patients with stage I disease and have identified several prognostic factors, including histologic type, tumor grade, depth of myometrial invasion, presence of lymphovascular space invasion, and peritoneal cytology.3–8 The study cohorts were heterogeneous, often grouping different histologies, all stage I and occasional stage II, and patients receiving a variety of adjuvant treatments, including chemotherapy and/or radiation therapy. However, the prognostic factors predictive of disease recurrence in patients with low-grade, non-myoinvasive, lymphovascular space invasion-negative endometrioid endometrial cancers have yet to be defined.
More recently, the Cancer Genome Atlas Network identified four molecular subtypes of endometrial cancer with prognostic implications: POLE-ultramutated, MSI-hypermutated, copy-number low, and copy-number high.9 This molecular classification has been proposed as a tool to help stratify risk in low-risk endometrial cancer.10 In particular, CTNNB1 exon 3 hotspot mutations have been suggested as likely drivers of a more aggressive subtype of low-grade, early-stage endometrioid endometrial cancers.11 Several retrospective studies have reported that patients with uterine-confined disease whose tumors harbor a somatic CTNNB1 exon 3 mutation have worse clinical outcomes compared with patients whose tumors are CTNNB1 wild-type.12–14
Here, we sought to evaluate the characteristics of patients with recurrent low-grade, non-myoinvasive (‘ultra-low risk’) endometrioid endometrial cancers. We explored the clinical characteristics of these patients, as well as the molecular profiles of recurrent and non-recurrent ultra-low risk tumors. The ability to accurately identify these patients early in their clinical course may lead to different decisions regarding adjuvant therapy, and an improved clinical outcome.
Methods
Case Selection
This study was approved by our institution’s Institutional Review Board. Our Institutional Database and the Gynecology Disease Management Team Database were queried for patients with International Federation of Gynecology and Obstetrics (FIGO) tumor grade 1, pathologic stage I endometrioid endometrial cancers who underwent surgery at our institution between January 2009 and February 2017. Staging was assigned using the FIGO 2009 staging system. All patients included in this study had stage IA, grade 1 endometrioid endometrial cancers without myometrial or lymphovascular space invasion. As pelvic fluid cytology is not part of the 2009 staging criteria, patients with both positive and negative cytology were included. Lymph node assessment was not required for inclusion. Patients with synchronous ovarian cancers and/or a follow-up time of less than 12 months were excluded. As surveillance visits are scheduled in 3- to 6-month increments, a minimum follow-up of 12 months captures at least two surveillance visits and improves the likelihood of identifying recurrent disease. All the endometrioid endometrial cancers included in this study were reviewed by an expert gynecologic pathologist.
Electronic medical records were queried for demographics, clinical characteristics, cancer treatment, and follow-up. Time to recurrence was calculated from hysterectomy until date of pathologic proven recurrence. Overall survival was calculated from date of primary surgery until death or last follow-up.
Targeted Massively Parallel Sequencing, Microsatellite Instability, and Mismatch Repair Deficiency Analyses
DNA mismatch repair (MMR) protein status was obtained from pathology reports/electronic medical records. Immunohistochemical analysis of the MMR proteins—MLH1, MSH2, PMS2, MSH6—was performed, as previously described.15 Endometrioid endometrial cancers with MLH1 and PMS2 deficiency by immunohistochemistry were subjected to MLH1 promoter methylation analysis.16 DNA from formalin-fixed paraffin-embedded tumors and from matched normal tissue or blood from all nine available cases with recurrent disease and from 27 non-recurrent endometrioid endometrial cancers were subjected to MSK-IMPACT (Memorial Sloan Kettering-Integrated Mutation Profiling of Actionable Cancer Targets) sequencing, targeting 341–468 cancer-related genes.17 18 The primary tumor was subjected to sequencing for both recurrent and non-recurrent cases. Sequencing data analyzes were performed using validated bioinformatics approaches, as previously described.19 20 All available primary tumors that developed recurrent disease were subjected to sequencing. To minimize bias in comparing genomic alterations in recurrent and non-recurrent low-risk endometrioid endometrial cancers, all non-recurrent tumors that were subjected to genomic profiling were included in analyzes. For the quantification of microsatellite instability (MSI), MSIsensor was used as described by Niu et al.21 Samples with MSIsensor scores ≥10 were deemed MSI-high, MSIsensor scores ≥3 to<10 indeterminate, and MSIsensor scores <3 microsatellite stable (MSS), as described.19 21
Statistical Analyses
Statistical analyses were performed using SPSS software, version 25.0 (IBM, Armonk, NY, USA). Number of mutations between groups were compared using the Mann-Whitney U test, and mutational frequencies using Fisher’s exact test, two-tailed. Dichotomous outcomes were compared with χ 2 test, except when the cell sizes were less than 10, in which case the Fisher’s exact test was used. Survival was calculated using the Kaplan-Meier method. Results were considered statistically significant if p<0.05 or if 95% CIs did not contain 1.0.
Results
Clinical Features of Ultra-low Risk Endometrioid Endometrial Cancers
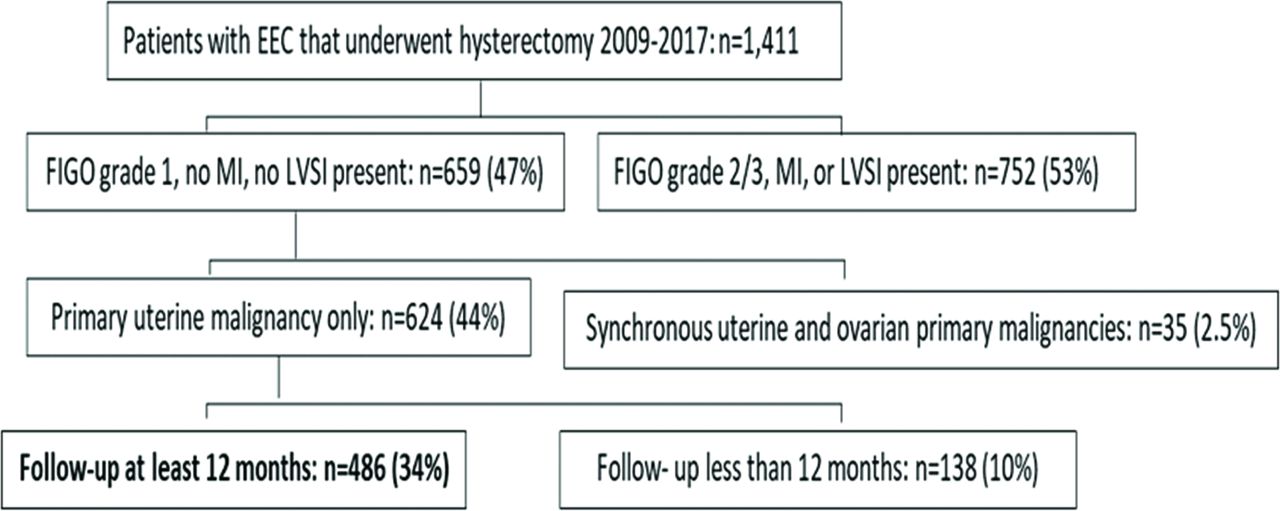
A total of 1411 women underwent hysterectomy for pathologic stage I endometrioid endometrial cancers at our institution (Figure 1). There were 659 (47%) patients with grade 1 endometrioid endometrial cancers, no myometrial invasion, or lymphovascular space invasion. Thirty-five (2.5%) of these patients were excluded because they had synchronous ovarian cancer; an additional 138 (10%) were excluded because they had less than 12 months follow-up post-surgery. In total, 486 (34%) patients were included in this study.
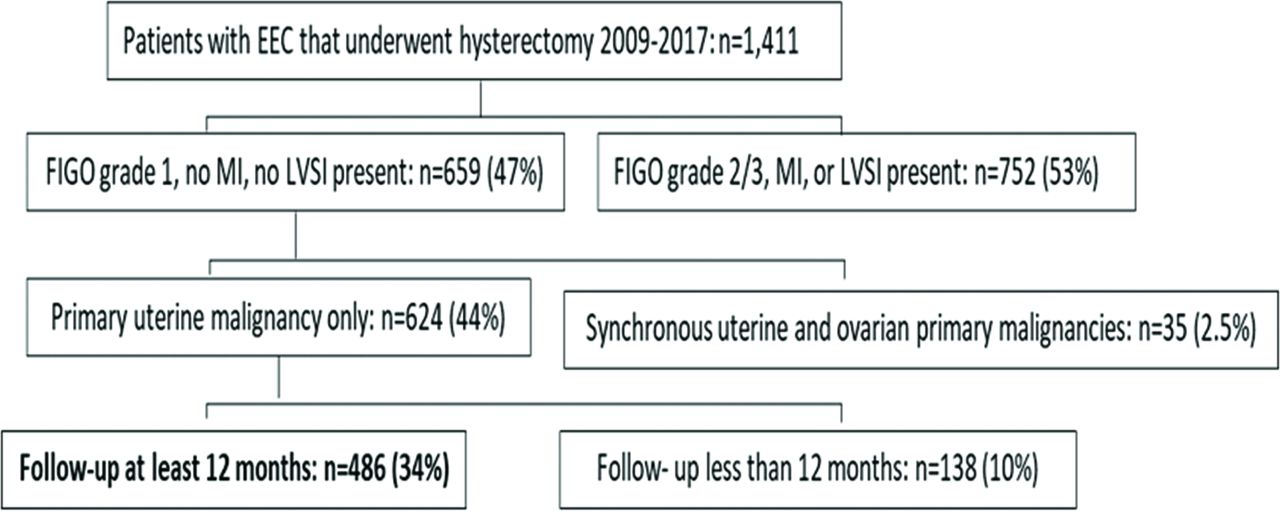
Patient selection for inclusion in study. Patients included had International Federation of Gynecology and Obstetrics (FIGO) grade 1 endometrioid endometrial adenocarcinoma (EEC), no myometrial invasion (MI), and no lymphovascular space invasion (LSVI). Synchronous ovarian malignancy was an exclusion criterion. Pelvic/peritoneal fluid cytology positive for carcinoma was not an exclusion criterion.
Median age at hysterectomy was 58 (range 28–91) years (Table 1). Most patients identified as White (n=403, 83%), 17 (4%) identified as African American, 38 (8%) as Asian, 2 (0.4%) as Hispanic, 11 (2%) as Other, and 15 (3%) did not answer the question. Median body mass index (BMI) at time of hysterectomy was 31 (range 16–69) kg/m2.
Clinicopathologic features of the ultra-low risk endometrioid endometrial cancer patients included in the study
Most patients underwent minimally invasive surgery: 107 (22%) patients had total laparoscopic hysterectomy and 345 (71%) had robotic-assisted total laparoscopic hysterectomy. An additional 34 (7%) patients underwent a total abdominal hysterectomy. Sentinel lymph node mapping and excision was performed in 345 (71%) patients, and 106 (22%) had total pelvic lymph node dissection. Thirty-five (7%) patients did not undergo lymph node analysis. In these cases, the decision to not remove lymph nodes was based on the absence of myoinvasion, as seen on intra-operative frozen section.22 Pelvic fluid cytology was obtained for 432 (89%) patients and was positive for carcinoma in 21 (4%). No patient received adjuvant therapy following surgery.
Clinical Features of Recurrent Ultra-low Risk Endometrioid Endometrial Cancers
Of the 486 endometrioid endometrial cancers patients included in this study, 14 (2.9%) developed recurrences (Table 2). All recurrences were confirmed by an expert gynecologic pathologist. Median follow-up for ultra-low risk endometrioid endometrial cancers patients who developed recurrences (n=14) was 50.5 (range 20–116) months, compared with 34.0 (range 12–116) months for non-recurrent cases (n=472, p=0.01). For recurring patients, median time until cancer recurrence was 13 months (95% CI, 0 to 31.3). Recurrent patients were older than non-recurrent patients (median 65 years, range 40–84, p=0.025 vs median 57.5 years, range 28–91) and had a lower median BMI (median 27.6 kg/m2, range 20.9–30.8 vs median 31.2 kg/m2, range 16.4–68.6, p≤0.001) (Table 1). Of note, no other clinical and pathologic characteristics assessed, including type of hysterectomy, type of lymph node dissection, the presence of positive pelvic/peritoneal cytology, or tumor DNA MMR proficiency differed between ultra-low risk endometrioid endometrial cancers with or without recurrences.
Clinicopathologic characteristics of the 14 endometrioid endometrial cancer patients with tumor recurrence
All recurrences were of endometrioid histology, akin to the primary tumors, and the majority of recurrences were of low tumor grade: 11 (79%) grade 1, 2 (14%) grade 2, and 1 (7%) grade 3. Eleven (79%) patients had single site recurrence and 3 (21%) had multi-site recurrence. For those with single site recurrence, eight had a vaginal cuff recurrence, two pelvic mass (other than lymph node), and one had lung nodule recurrence (Table 2). The three patients with endometrioid endometrial cancers with multisite recurrence had a combination of local and distant disease (one patient had pelvic lymph node involvement). Recurrences were treated with radiation therapy alone (n=6), chemotherapy alone (n=1), or multimodal therapy (combination of chemotherapy and/or radiation therapy and/or surgery and/or hormonal therapy, n=7). Three patients had progressive or recurrent disease following completion of treatment for their first recurrence. At last follow-up, 12 (87%) patients were alive, of whom 4 (33%) had active disease. Median overall survival was not reached for the group.
DNA MMR Protein Analysis
Immunohistochemisty of the DNA MMR proteins MLH1, MSH2, MSH6 and PMS2 was available for 211/486 (43%) endometrioid endometrial cancers. The majority of ultra-low risk endometrioid endometrial cancers (158/211, 75%) were found to be DNA MMR-proficient, and 53/211 (25%) tumors displayed loss of DNA MMR protein expression. Of the 53 DNA MMR-deficient endometrioid endometrial cancers, 24 (45%) were MLH1-hypermethylated. The majority (49/53, 92%) of the patients with MMR-deficient tumors underwent germline mutation testing, and 10 (19%) were found to have Lynch syndrome. Of the 14 patients who experienced a recurrence, MMR protein immunohistochemistry was available for 5 (36%); of these, three displayed loss of MMR protein expression and MLH1-hypermethylation.
Mutational Profiles and MSI Status of Ultra-low Risk Endometrioid Endometrial Cancers
A series of 9 (n=14, 64%) recurrent and 27 (n=472, 6%) non-recurrent endometrioid endometrial cancer tumors underwent molecular profiling. There were no differences in clinicopathologic factors between patients who underwent tumor profiling and those who did not (median age, median BMI, race, type of surgical approach, type of lymph node assessment, and pelvic washing status; p>0.05, respectively). Except for patient race, clinicopathologic characteristics did not differ between those with and without a recurrence (Table 3). First, we assessed whether there was a difference in the mutational profiles between ultra-low risk endometrioid endometrial cancers that did recur compared with those that did not. Mutational profiling of primary tumors from nine recurrent and 27 non-recurrent endometrioid endometrial cancers patients revealed a similar mutation burden, with recurrent endometrioid endometrial cancers harboring a median of 5.9 (range 3.7–180.6) and non-recurrent endometrioid endometrial cancers a median of 5.1 (range 0–178.3) non-synonymous somatic mutations (p=0.52). The majority of ultra-low risk endometrioid endometrial cancers were MSS as defined by MSIsensor, and no differences between the recurrent versus non-recurrent groups were found (recurrent endometrioid endometrial cancers: 6/9 MSS, 2/9 MSI-indeterminate, 1/9 not assessable; non-recurrent endometrioid endometrial cancers: 25/27 MSI-stable, 1/27 MSI-indeterminate, 1/27 not assessable).
Clinicopathologic features of the ultra-low risk endometrioid endometrial cancer patients that underwent molecular profiling (n=36)
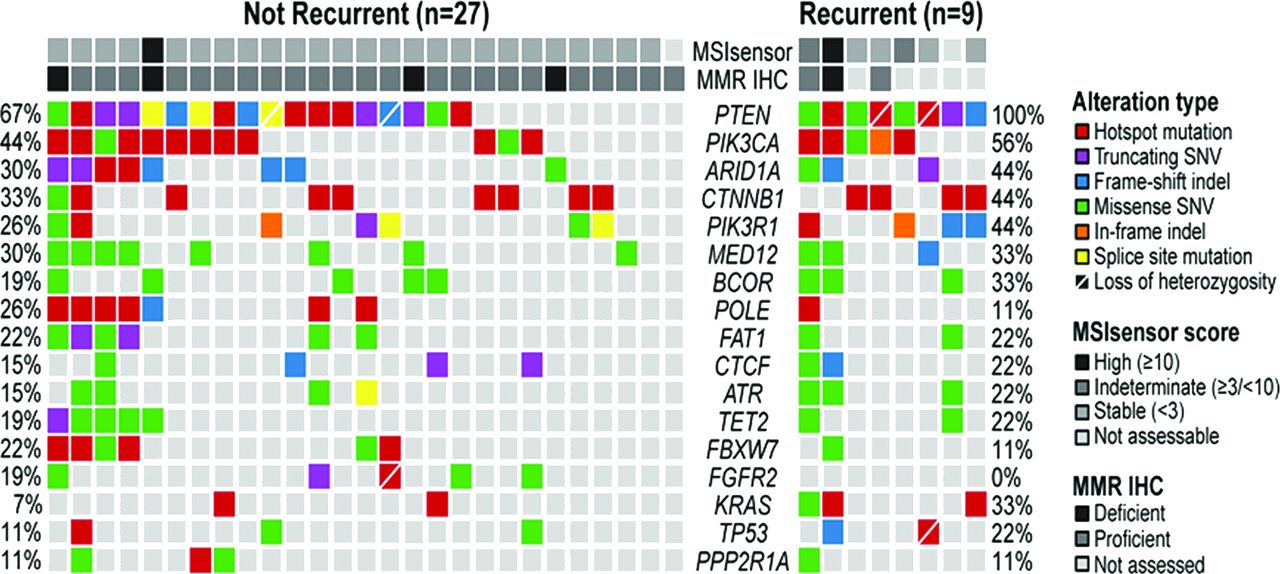
Mutational analysis revealed that PTEN and PIK3CA were the most frequently mutated genes in both groups, with PTEN mutations being present in 100% (9/9) of recurrent and 63% (17/27) of non-recurrent endometrioid endometrial cancers (p=0.04), and PIK3CA mutations in 56% (5/9) of recurrent and 44% (12/27) of non-recurrent endometrioid endometrial cancers (p=0.71) (Figure 2). Of interest, there were six tumors with POLE exonuclease domain mutations, including 1/9 recurrent (11%) and 5/27 non-recurrent (19%) endometrioid endometrial cancers (p=1.00). Mutations included p.A456P, p.V411L, p.P286R, p.F367V, and p.P436R, which have been previously described as hotspot or pathogenic mutations and are associated with an ultramutator phenotype.18 23–25
{kind=link}
{kind=link}
Mutational profiles of low-grade, non-invasive endometrioid endometrial cancers with and without recurrences. Targeted massively parallel sequencing was performed for 27 non-recurrent and nine recurrent endometrioid endometrial cancers. All samples were from the primary tumor, regardless of recurrence status. The most recurrent genes affecting 341–468 cancer-related genes are shown. Mutation types are color coded by the legend. Note that none of the mutations were statistically significantly different between non-recurrent and recurrent ultra-low risk endometrioid endometrial cancers. IHC, immunohistochemistry; MMR, mismatch repair; MSI, microsatellite instability; SNV, single-nucleotide variant.
None of the other genes analyzed were mutated at statistically significant frequencies between the two groups. This included TP53, seen in 22% (2/9) recurrent and 11% (3/27) of non-recurrent tumors (p=0.58) and CTNNB1 exon three hotspot mutations, which were found in 44% (4/9) of recurrent endometrioid endometrial cancers and 30% (8/27) of non-recurrent endometrioid endometrial cancers (p=0.44).
Discussion
While patients diagnosed with low-grade, early-stage endometrioid endometrial cancer have an overall excellent prognosis, there is a subset of patients who will experience a recurrence. In our study, the rate of cancer recurrence in this selected low-risk cohort of grade 1 stage I endometrioid endometrial cancers without lymphovascular space invasion or myoinvasion was 2.9%. We did not identify any distinctive clinical characteristics that were unique to the patients who had a cancer recurrence.
Previous work has focused on the identification of molecular markers associated with recurrence in endometrioid endometrial cancers. For example, Liu and colleagues initially identified a subset of patients whose tumors harbored a CTNNB1 hotspot mutation in exon 3 and had a worse clinical outcome than those whose tumors lacked the mutation.11 This initial clinical cohort comprised patients with all grades and all stages of disease. The molecularly-selected more aggressive subtype of endometrioid endometrial cancer was seen in younger patients, with low-grade (90% grade 1/2) and early-stage (88% stage I/II) disease. This early finding was then validated by Kurnit and colleagues in patients with low-grade (grade 1/2) and early-stage (stage I/II) endometrioid endometrial cancers,12 in whom a CTNNB1 exon 3 mutation was associated with worse outcome. Of interest, the authors noted that patients with endometrioid endometrial cancers harboring the mutation were more likely to have tumors with pathologic characteristics associated with a lower risk of recurrence, including lower FIGO grade, less deep myometrial invasion, and less lymphovascular space invasion. The association between shorter survival and endometrioid endometrial cancer with a CTNNB1 mutation was also noted in a 2019 report by Costigan and colleagues.13
Despite published literature demonstrating that low-grade, early-stage endometrioid endometrial cancers with CTNNB1 mutation are more likely to have worse cancer-related outcomes, we identified a similar frequency of CTNNB1 exon 3 hotspot mutations between endometrioid endometrial cancers in patients with a cancer recurrence and endometrioid endometrial cancers in patients without recurrence. Importantly, we focused on evaluating an ultra-low risk cohort of patients with no myometrial invasion or lymphovascular space invasion.
While it is notable that, in our cohort, the median follow-up time for patients without a recurrence was 17 months less than for patients with a recurrence (34 vs 50.5 months), for those patients who did recur, the median time until cancer recurrence was 13 months (95% CI 0 to 31). Given that the majority (68%–100%) of all recurrences in endometrioid endometrial cancers are diagnosed by 3 years, the median follow-up time of 34 months for the non-recurrent cohort is informative.26
Our study is limited by its retrospective nature and the small number of tumors that were subjected to sequencing, given the rarity of ultra-low risk endometrioid endometrial cancers that recur. As a historic cohort, MMR protein proficiency data were unavailable for over half of the samples, limiting possible MMR-proficiency analysis. Further, our results are subject to a degree of ascertainment bias—all patients with non-recurrent malignancies were consented to tumor genomic sequencing at time of their diagnosis (offering testing to newly diagnosed patients has been the standard at our institution since 2016), while patients who experienced a recurrence had tumor testing either because they had a recurrence or for the purposes of this report. However, the samples included in the current study were homogeneous from a clinical and pathologic perspective: all grade 1, non-invasive tumors with no lymphovascular space invasion. Therefore, the non-recurrent samples that had undergone genomic profiling and were included in this report were considered an appropriate representation for the non-recurrent tumors in the cohort. Finally, because of the small number of recurrent tumors that were sequenced, we could not perform any intra-group comparisons (for example, comparing the tumor genomic profile in patients that had a single-site recurrence with those that had multi-site recurrences).
Although the evidence available to date supporting CTNNB1 mutation as a poor prognostic indicator is compelling, all data reported thus far are retrospective in nature. We did not identify a greater frequency of the CTNNB1 mutation in our ultra-low risk cohort. Based on our findings, tumor mutational sequencing analysis for patients with non-invasive, low-grade endometrial cancer currently does not seem to substantially contribute to the clinical management of these patients. However, larger studies are warranted, and we anticipate the results of PORTEC-4a (CT03469674), which will help evaluate the utility of treating patients based on molecular subtyping rather than clinicopathologic staging.27 At this time, further research is warranted to identify molecular markers that distinguish the group of patients with extremely low-risk disease who experience cancer recurrence.
Supplemental material
References
Footnotes
Twitter @leitaomd
Contributors MS, JM: conception and design; analysis and interpretation of data; drafting of article; revising article critically for important intellectual content; final approval of version to be published; agree to be accountable for all aspects of the work. NF, KAC: analysis and interpretation of data; drafting of article; final approval of version to be published; agree to be accountable for all aspects of the work. SSKL, CS, RAS, KA, EMDS, APMS, ML, GG, PS, NRA-R: interpretation of data; revising article critically; final approval of version to be published; agree to be accountable for all aspects of the work. BW: analysis and interpretation of data; drafting of article; revising article critically for important intellectual content; final approval of version to be published; agrees to be accountable for all aspects of the work.
Funding This study was funded in part through the NIH/NCI Support Grant P30 CA008748. Dr Weigelt is funded in part by the Breast Cancer Research Foundation, Cycle for Survival, and Stand Up to Cancer.
Disclaimer Dr Abu-Rustum reports grants from Stryker/Novadaq, grants from Olympus, grants from GRAIL, 283 outside the submitted work. Dr Cadoo reports other* from Astra Zeneca, other** from Syndax Pharmaceuticals, outside the submitted work. (*Travel, accommodation, meal; institutional support for therapeutic trial; **institutional support for therapeutic trial.) Dr Leitao is an ad hoc consultant for Intuitive Surgical Inc., outside the submitted work. Dr Soslow reports personal fees from Ebix/Oakstone*; personal fees from Cambridge University Press**; personal fees from Springer Publishers**; personal fees from Roche***, outside the submitted work. (*Preparation of recorded lectures; **royalties; ***one lecture.)
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.