Article Text

Abstract
Objectives Globally, cervical cancer is a leading cause of death. Lack of international consensus on standard-of-care (SoC) treatment for locally advanced cervical cancer (LACC) (Stages IB2-IVA) may contribute to inconsistent treatment. We compared LACC treatment recommendations from international guidelines.
Methods Literature databases (1999–2020), national authority websites, and bibliographies were searched for English-language cervical cancer guidelines, with no restriction on geography. Included guidelines were treatment-focused and represented the latest update.
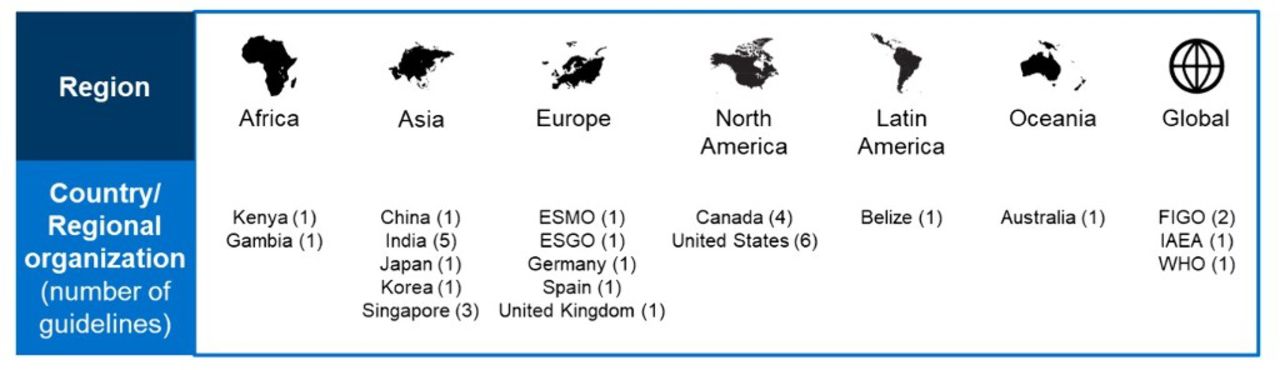
Results Thirty-four guidelines were identified (figure 1), with the majority updated 2016–2021. Seven provided only high-level overviews of treatment modalities, and were excluded. Treatment recommendations were based on FIGO 2009 (n=20 guidelines), FIGO 2018 (n=6), and TNM (n=1) staging. For Stage IB2-IIA2, treatment options were diverse within/between guidelines and included radical hysterectomy (RH), cCRT, radiotherapy. The most common recommendation was a choice of RH/cCRT (IB2 n=12; IIA n=18), with variable treatment selection criteria between guidelines. Adjuvant cCRT/radiotherapy after RH was advisable with high/intermediate recurrence risk (n=23). For Stage IIB-IVA, cCRT was SoC, with ≥67% guideline consensus. However, for Stage IIB, surgery was SoC in Japan/Germany. Ten guidelines offered Stage IVA treatment alternatives. Kenya/Gambia recommendations were distinct, offering chemotherapy alone and/or excluding cCRT. Consensus cCRT regimen was weekly cisplatin (40mg/m2) concurrent with external beam radiotherapy followed by brachytherapy; for 6 guidelines it was unclear if cCRT included brachytherapy.

{kind=link}
Conclusions With few exceptions, there is international consensus for cCRT as SoC for Stage IIB-IVA LACC, whereas recommendations for Stage IB2-IIA disease varied. Funding: AstraZeneca