Article Text

Abstract
Introduction/Background*The most effective treatment strategy for FIGO stage IV endometrial cancer (EC) is currently unclear. Cytoreductive surgery is considered to improve overall survival, but this is based on small series. Further insight in the heterogeneity of this patient population’s tumours and the impact of the completeness of surgery is lacking.
This study aimed to determine overall survival benefit of cytoreductive surgery in patients with FIGO stage IV endometrial cancer that underwent complete, optimal or incomplete cytoreduction compared to no surgery at all.
Methodology We performed a retrospective national multicenter cohort study analyzing retrospective data from Jan 1, 2000, to Dec 31, 2018, from patients with FIGO stage IV EC, treated in five different hospitals in The Netherlands. Patients who underwent surgery for recurrent EC or patients with a uterine sarcoma were excluded from the analysis. Kaplan Meier analysis was performed to estimate overall survival and multivariable analysis was performed with the Cox proportional hazard model. Molecular classification is currently being conducted to evaluate correlation between molecular EC class and outcome.
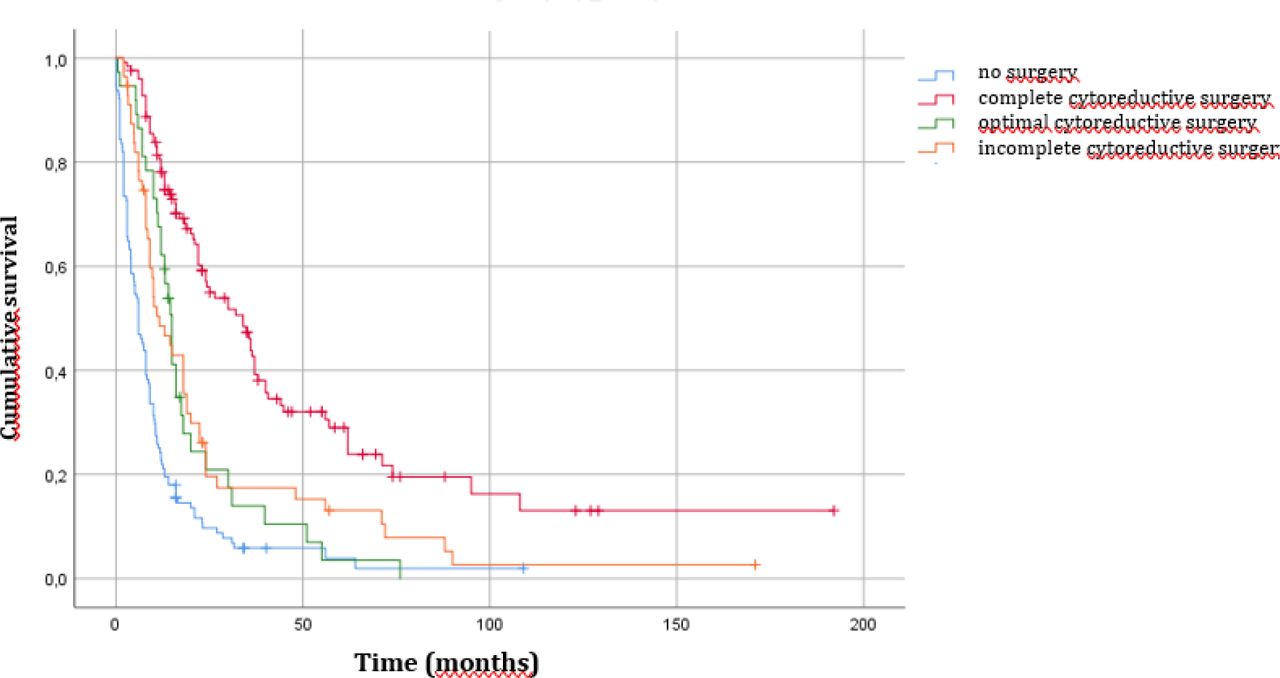
Result(s)*Characteristics of the 347 patients included are shown in table 1. The most common histological subtype was endometrioid adenocarcinoma (146 of 347, 42,1%). Complete cytoreductive surgery was achieved in 126 of 347 patients (36.3%), while in 37 patients (10.7%) optimal cytoreductive surgery was achieved and in 56 patients (16,1%) incomplete cytoreductive surgery. 128 patients (36,9%) did not receive surgical treatment. Median overall survival was 13 months (figure 1). Complete cytoreductive surgery led to an OS of 34 months (p=0.00, HR 0.34, 95% CI: 0.26-0.45%) compared to 15 months for patients who underwent optimal cytoreductive surgery and 11.6 months for patients who underwent incomplete cytoreductive surgery. Patients who did not receive surgical treatment had a median OS of 6 months. If possible, the molecular EC classification data will be presented at the ESGO congress.

{kind=link}
Kaplan-Meier plots showing the overall survival curves of patients with stage IV endometrial cancer that underwent complete, optimal or incomplete cytoreductive surgery or no surgery at all
Patient characteristics
Conclusion*Complete cytoreductive surgery leads to an extended overall survival in patients with FIGO stage IV EC in comparison to optimal or incomplete cytoreductive surgery or to no surgery at all. Our data support omission of surgical treatment when complete cytoreduction cannot be achieved.