Article Text

Abstract
Introduction/Background*The clinical presentation of advanced USC may overlap significantly with that of serous carcinoma of tubo-ovarian origin. Differentiation facilitates patient counselling; guides choice of imaging; accurately stages; and fully informs MDT discussion – bearing in mind primary surgery as the treatment of choice for the less chemo-sensitive USC.
Methodology Cases of serous carcinoma initially presumed of tubo-ovarian origin, but confirmed on final histopathology as USC, were identified and patient care records reviewed retrospectively.
Three cases were identified Mean age 75.7years. All presented with pain, distension but no post-menopausal bleeding. Each had an elevated CA125. Initial CT reported disseminated disease. Image-guided biopsy reported serous carcinoma. All three specimens were positive for p16, p53 and CA125; but only two WT1 positive (with focal/weak pattern) and one WT1 negative. After MDT discussion, all patients underwent neo-adjuvant chemotherapy for presumed stage IIIc/IV tubo-ovarian serous carcinoma. Delayed primary surgery achieved R0 in all cases. Whilst final histopathology confirmed serous carcinoma, the diagnosis was amended to USC in each – arising from an endometrial polyp (mean size 16mm) in all three women.
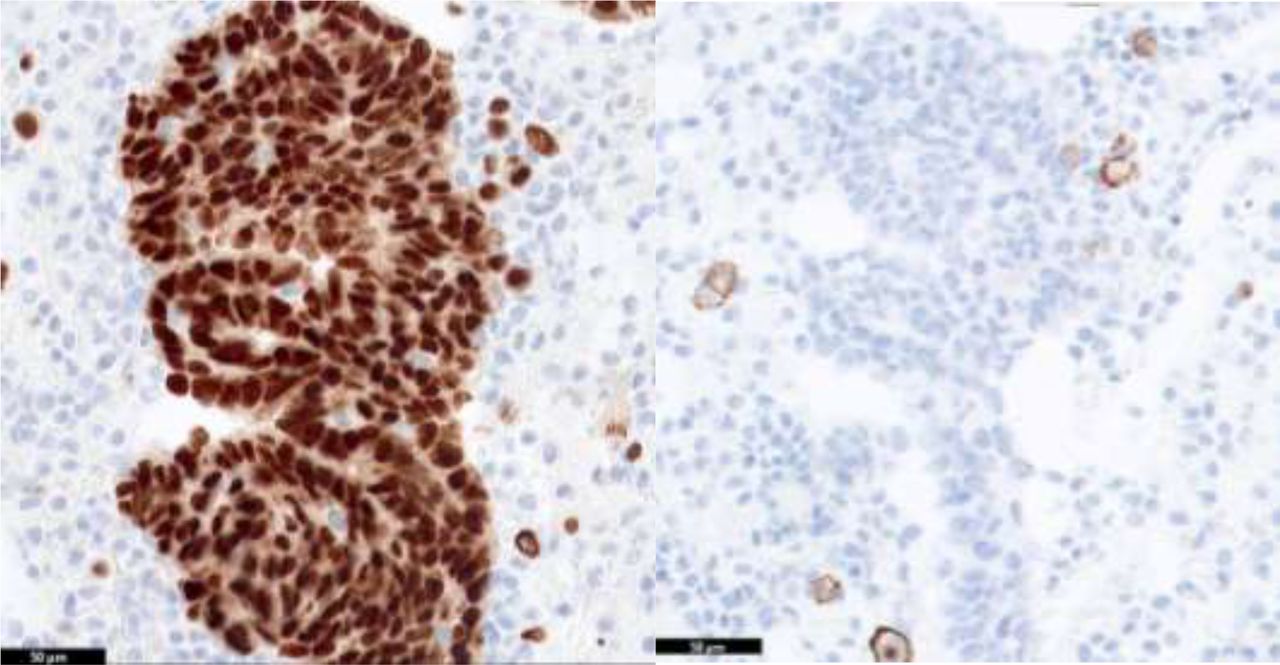
Diffuse strong WT1 staining of tubo-ovarian HGSC v focal weak WT1 staining of USC
{kind=link}
{kind=link}
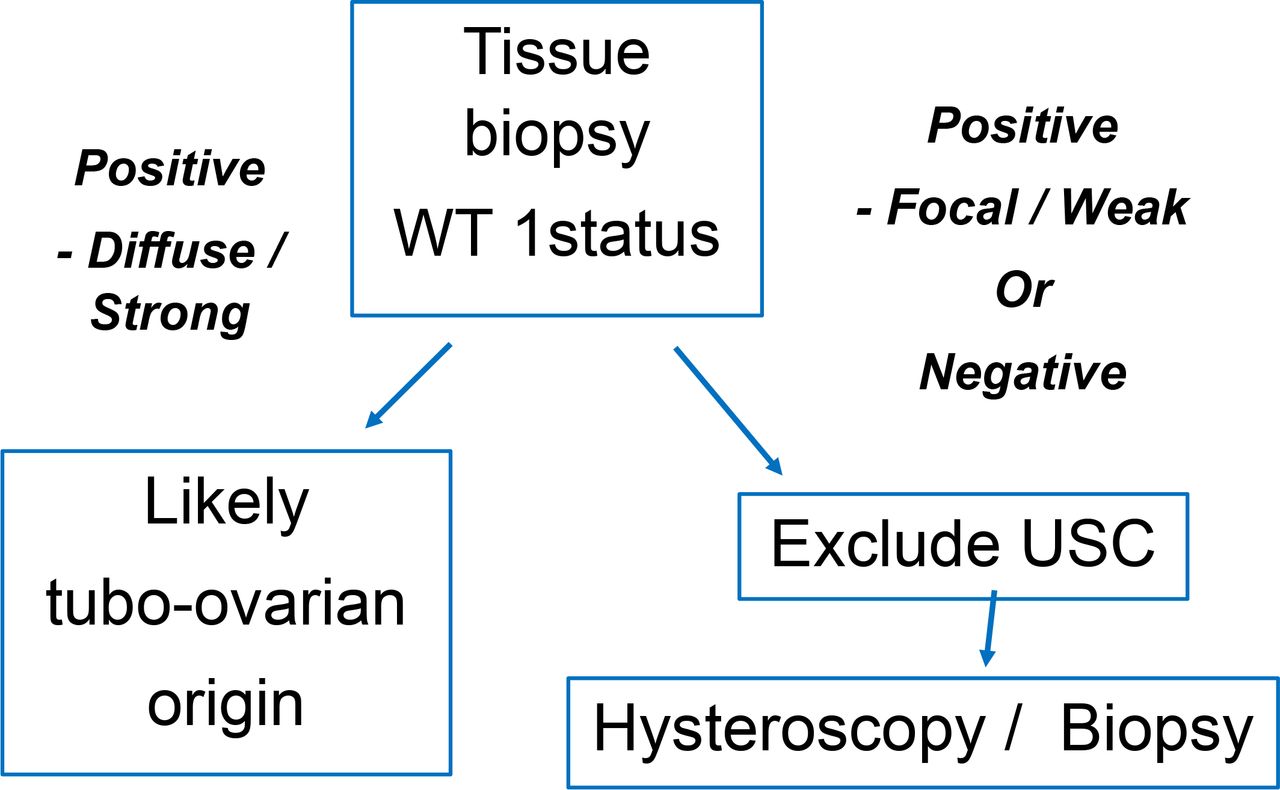
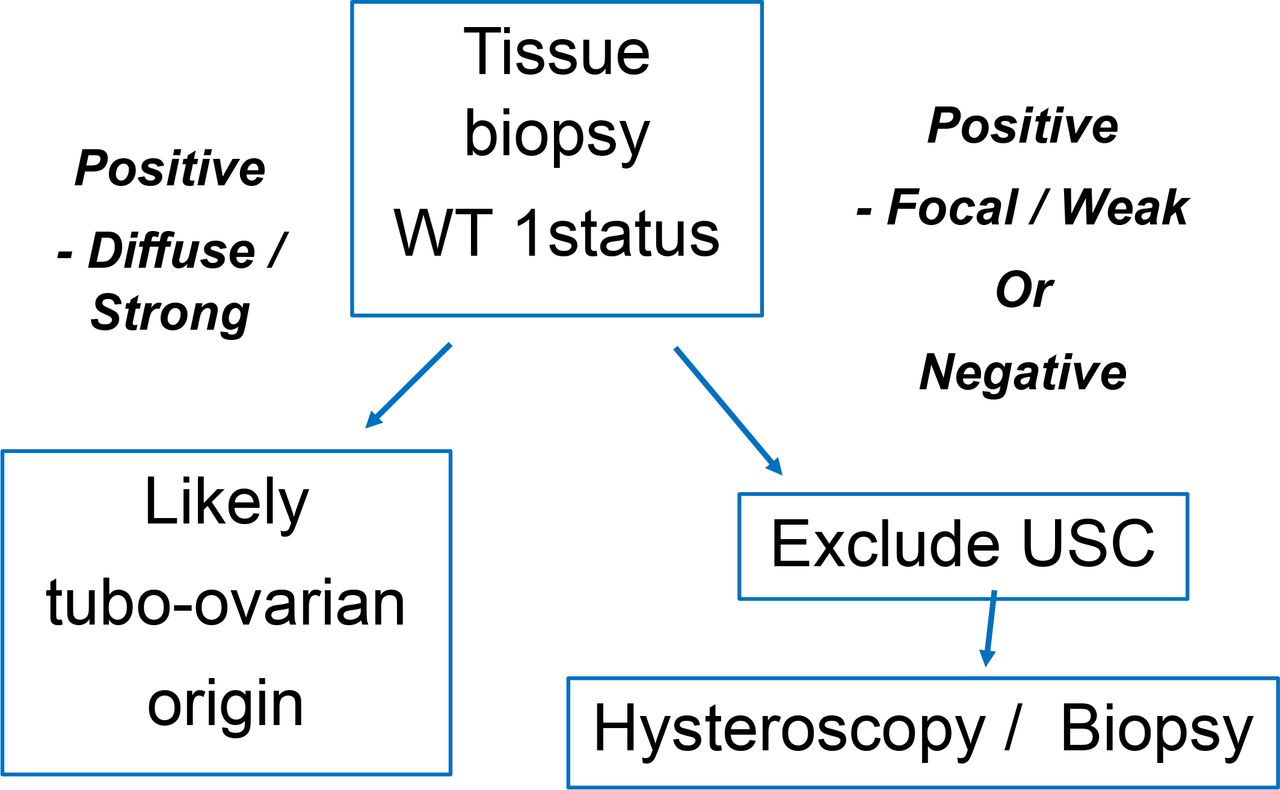
Suggested pre-operative algorithm to distinguish USC v HGSC of tubo-ovarian origin
Conclusion*Whilst several immunohistochemical markers are universal between the tumour types, the literature suggests that the majority (94.7%) of serous carcinomas of tubo-ovarian origin exhibit positive WT1; compared to only 10-20% of USC. Further distinction arises in the pattern of WT1 positivity – strong/diffuse in tubo-ovarian versus focal/weak in the cross-over USC group. This correlates with our case series. We suggest that in disseminated serous carcinoma with negative WT1 or focal/weak positivity pre-operative hysteroscopy/biopsy is considered. Whilst this may not always alter management, for patients on the border of suitability for primary surgery a preparedness to exert maximal surgical effort may be favoured on identifying USC.