Article Text

Statistics from Altmetric.com
INTRODUCTION
Ureteric injury, is a common complication following gynecological, urological, and colorectal procedures. Risk factors associated with ureteric injury are anatomic variations, pelvic surgeries, laparoscopic procedures, previous radiation, adhesions, and malignancies.1 Most common approaches to repair of such injuries include primary anastomosis, uretero-ureterostomy, ureteral reimplantation, and Boari flap. Most of these procedures are done through a laparotomy approach. In this article we present a case of a delayed laparoscopic repair of a ureteric injury, after a cytoreductive surgery for ovarian cancer.
CASE
The patient is a 57-year-old woman who underwent primary cytoreductive surgery for stage IIIc high-grade ovarian cancer. The procedure involved open radical hysterectomy, bilateral salpingo-oophorectomy, omentectomy, and rectosigmoid resection with primary colorectal anastomosis. In addition, she had pelvic and retroperitoneal lymphadenectomy for enlarged para-aortic lymph nodes (Figure 1).
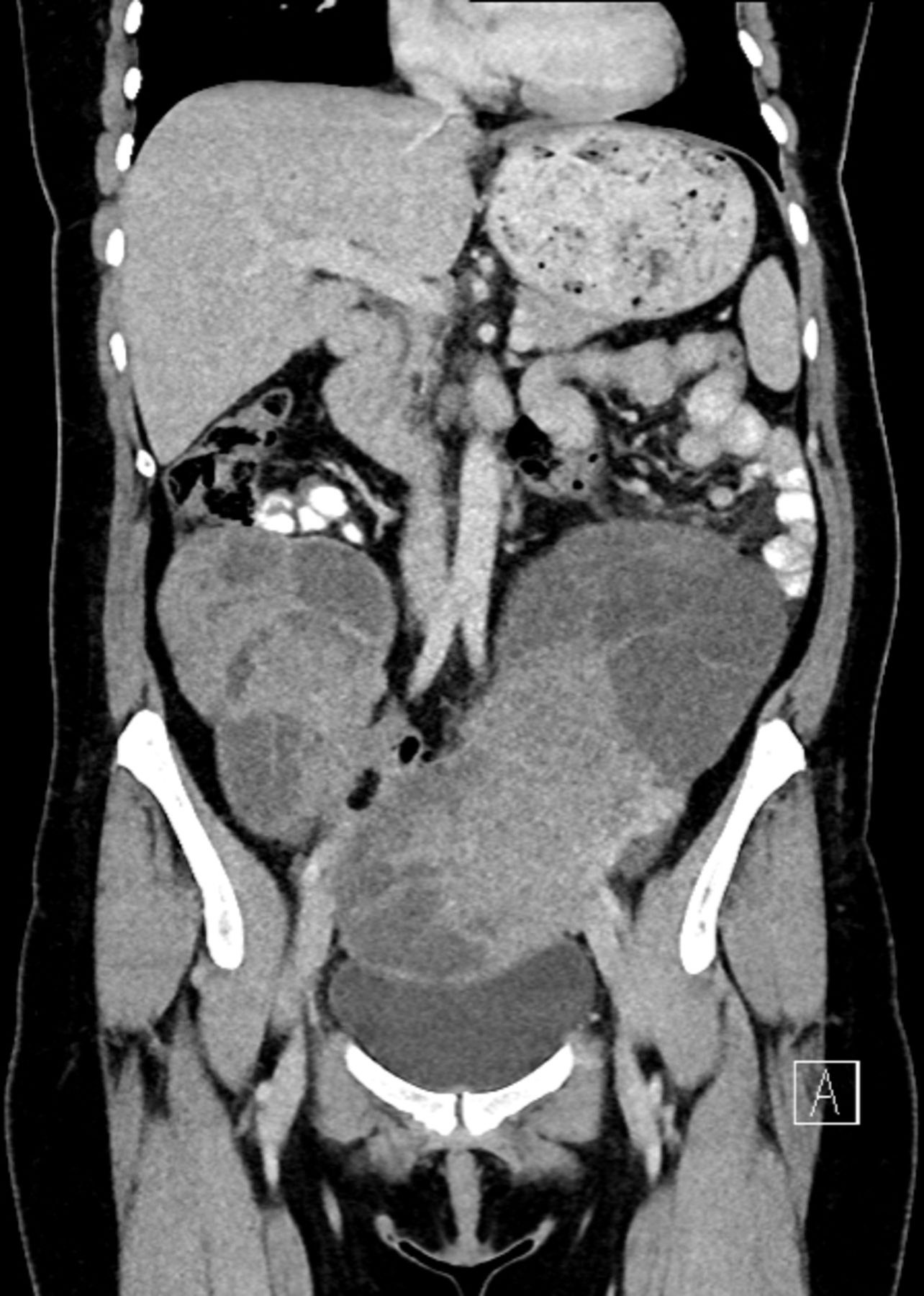
Coronal view of pre-operative CT abdomen/pelvis showing complex enlarged bilateral pelvic masses.
On post-operative day 10 she had a rise in urea and creatinine with decreased urinary output. A CT scan revealed left-sided hydronephrosis and retroperitoneal fluid collection (Figure 2), with delayed phase confirming ureteric injury. Interventional radiologically guided stenting was attempted but antegrade stenting could not be achieved. A nephrostomy tube was placed and a laparoscopic approach for repair of the ureter was performed.

Postoperative CT scan abdomen/pelvis coronal view showing hydronephrosis of the left kidney with proximal urinoma surrounding the ureter, consistent with ureteric injury.
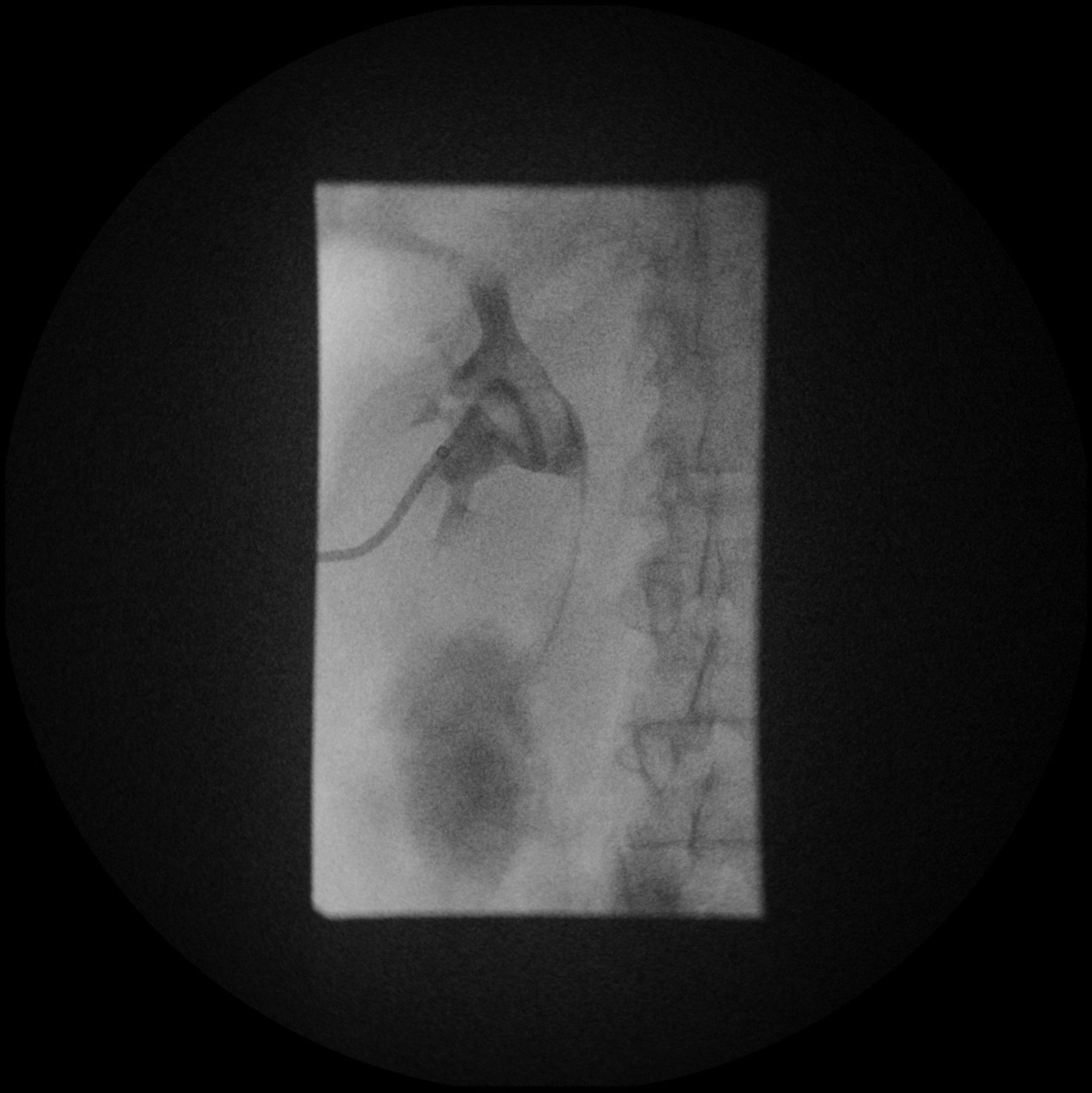
Fluoroscopic posterior view of the left kidney showing leakage from the left ureter; antegrade insertion of guide wire and JJ stent was not successful.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Laparoscopic view of proximal ureter found after injection of patent blue dye, and distal stump with JJ stent.
A 10 mm transumbilical port was inserted for camera access, and 4×5 mm ports for instrumentation in left and right lower quadrants. The retroperitoneal plane was re-dissected with caution in order not to tear the edematous tissue. A combination of blunt and sharp dissection was used. By opening the retroperitoneal space, the proximal and distal urinoma were identified.
The distal stump of the ureter was identified by finding the tied infundibulopelvic ligament, common iliac artery, and then following the internal iliac artery with the help of retrograde insertion of a JJ stent through cystoscopy. The proximal stump was identified by injecting 20 mL of diluted patent blue dye through the nephrostomy tube, and visualization of the leaking point through laparoscopy.
The first step was mobilizing the two ends of the ureter to get more length on either side, making sure to maintain the blood supply of the ureter to avoid ischemic necrosis. The tips of both stumps were incised and freshened, followed by spatulation of each side to avoid stricture formation. A stabilization stitch with 2/0 Vicryl suture in the proximal ureter helps to manipulate the ureter during suturing without damaging the adventitia. The JJ stent was advanced retrogradely to the proximal stump. The ureter was anastomosed using a 3/0 Monocryl interrupted suture at 3, 6, 9, and 12 o’clock positions.
Flo seal and HaemoCer were used on the surgical field to prevent bleeding and to help in the healing process.2 A Robinson drain was placed through the left lower quadrant port site. Finally, positioning of the JJ stent was confirmed with cystoscopy.
The intra-peritoneal drain was removed 4 days post-operatively, with minimal output, and on post-operative day 5 the catheter was removed and the patient was discharged. The nephrostomy tube was removed on post-operative week 2 and it was planned to remove the JJ stent 12 weeks post-operatively. The patient started chemotherapy on week 6 without any delay.
CONCLUSION
Ureteric injuries pose diagnostic and therapeutic challenges to the surgeons, especially after a major surgery. During investigations, it is crucial to choose the right investigation as urinary tract injury can be overlooked if a late-phase CT urogram is not requested from the radiologist.3 In oncological settings, the minimally invasive approach can facilitate early recovery and avoid delays in adjuvant treatments.
Ethics statements
Patient consent for publication
Footnotes
Twitter @FerasAbuSaadeh2
Contributors All authors participated in the operative procedure. The manuscript was drafted by DS and the final draft was reviewed and approved by all authors. The content was supervised and guaranteed by FAS.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.